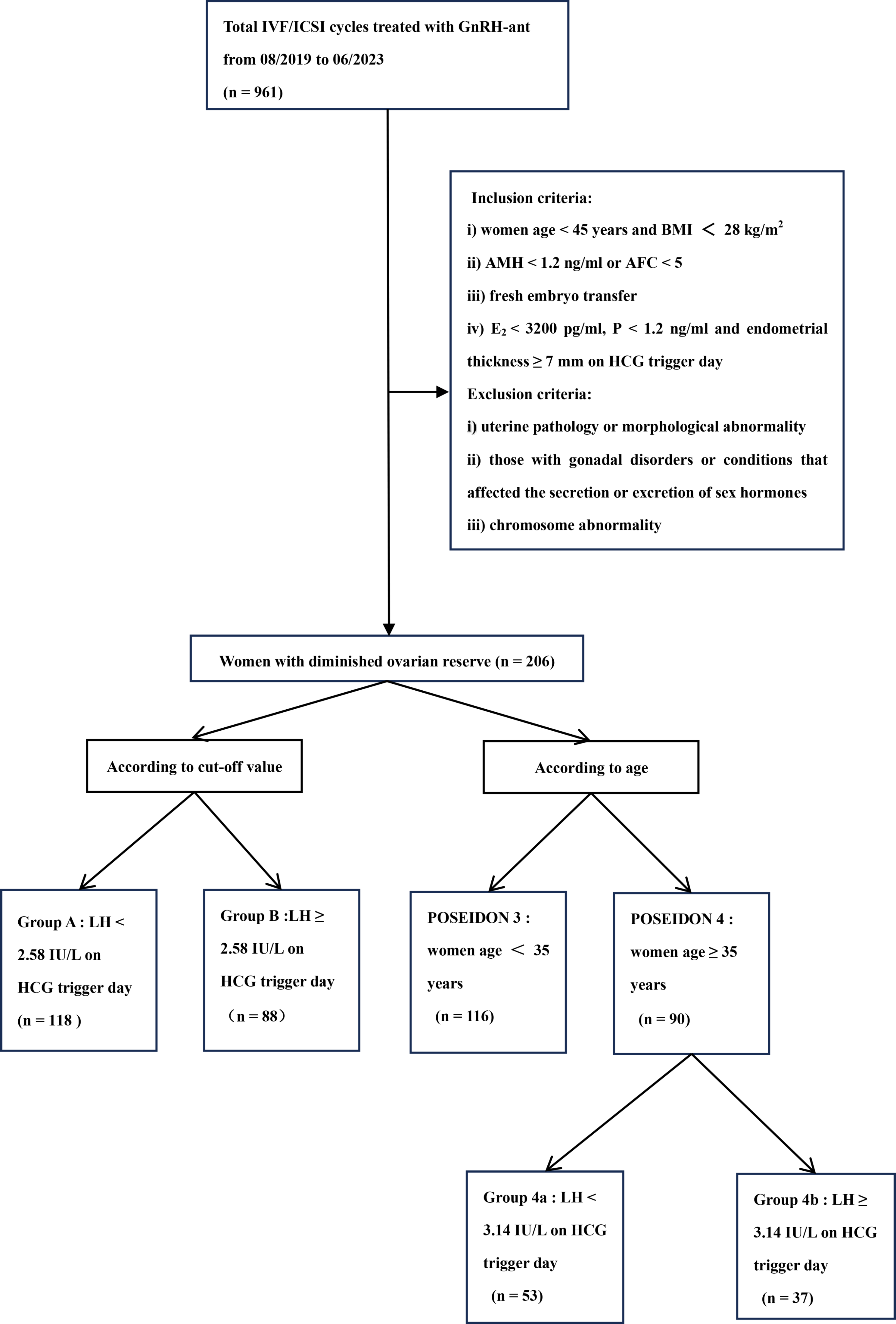
The purpose of this study is to investigate the effect of LHHCG on clinical pregnancy outcome in patients with DOR undergoing GnRH-ant protocol, and our results showed that LHHCG level was an independent factor affecting the clinical pregnancy outcome of patients with DOR. The HCG positive rate, embryo implantation rate, clinical pregnancy rate, and live birth rate in LHHCG < 2.58 IU/L group were significantly higher than those in LHHCG ≥ 2.58 IU/L group. However, in the study of Zhou et al., the live birth rate of the low LHHCG level group was lower than that of the high-level group among the NOR and PCOS population who used GnRH-ant protocol for fresh embryo transfer, while there was no significant difference in POR patients, which was different from our results [9]. This may be due to research population’s different inclusion criteria and grouping methods. The Bologna criteria was adopted in the study of Zhou et al., while the POSEIDON criteria was adopted in our study.
With the rapid development of ART, the GnRH-ant protocol has been commonly used around the world. In 2020, the European Society for Human Reproduction and Embryology (ESHRE) issued controlled ovarian hyperstimulation (COH) guidelines, which indicated that GnRH-ant protocol can be used as first-line treatment for normal ovarian response, diminished ovarian reserve, and patients with high ovarian response [15]. GnRH-ant protocol competitively blocks pituitary GnRH receptors and inhibits premature LH surge, which can prevent premature ovulation [16, 17]. Studies have indicated that there was no significant difference in clinical pregnancy rate and live birth rate between the GnRH-ant protocol and GnRH agonist protocol, and the number of high-quality embryos was similar. But compared to the GnRH agonist protocol, the GnRH-ant protocol had a lower implantation rate, clinical pregnancy rate and cumulative pregnancy rate [18,19,20]. Therefore, improving the implantation rate and pregnancy rate of patients is one of the key points in the application of the GnRH-ant protocol.
LH level is one of the factors that affecting COH and pregnancy outcome in GnRH-ant protocol [21]. LH controls gonadal function and plays a central role in regulating the complicated and delicate endocrine mechanisms of ovarian biology [22]. It controls the length and sequence of women’s menstrual cycle, including ovulation, the preparation of fertilized embryos for implantation into the uterus, and the production of estrogen and progesterone [23]. While clinical studies have shown that abnormal serum LH levels often occur in patients with DOR [24].
LH is essential for estrogen synthesis and maintaining the development of dominant follicles, and excessive stimulation of the ovaries by LH will adversely affect the normal development of pre-ovulatory follicles. Depending on the stage of development, exposure to inappropriately high concentrations of LH will interfere with communication between cumulus cells and granulosa cells, which affects the development of oocytes and may lead to follicular atresia or premature luteinization [25]. At present, the relationship between LHHCG and ovarian reserve and ovarian response in DOR patients is not completely clear. In our study, the LHHCG < 2.58 IU/L group had higher ovarian reserve and ovarian response than the LHHCG ≥ 2.58 IU/L group. The AFC and AMH, and the number of oocytes retrieved, number of mature oocytes in LHHCG < 2.58 IU/L group were more than those in LHHCG ≥ 2.58 IU/L group. It suggests that LHHCG may be an important indication of ovarian response. Xu et al. has confirmed that LHHCG ≥ 2 IU/L in GnRH-ant protocol is not conductive to follicles maturation and ovulation [26]. The study by Zhang et al. showed that in the follicular-phase long protocol, the LHHCG was negatively correlated with the number of oocytes retrieved, and the highest number of oocytes was retrieved when LHHCG ≤ 0.5 IU/L [27]. The optimal range of LHHCG in this study is different from that in previous studies, which may be due to the fact that this study only focused on DOR populations. This also suggests that conducting separate studies on different populations is beneficial to providing individualized treatment for patients during clinical ovulation induction.
The effect of LH on pregnancy outcomes and its mechanism are still not fully understood. Lucas et al. found that LH can inhibit the proliferation, migration, and differentiation of endometrial stem cells through Akt and ERK1/2 signaling pathways, and inhibit tissue regeneration-related functions through its cognate receptor LHR, thus reducing endometrial receptivity [28]. Besides, a rise in LH is often accompanied by a rise in progesterone levels, and the study has shown that LHHCG ≥ 8.46 IU/L may indirectly affect endometrial receptivity through the increase of progesterone, which may lead to the decrease of pregnancy rate in frozen embryo transfer cycle [8]. The increase of progesterone concentration not only damages endometrial receptivity but also affects embryo quality [29]. Since there was no significant difference in the high-quality embryo rate and the number of embryos transferred between the LHHCG < 2.58 IU/L group and the LHHCG ≥ 2.58 IU/L group in this study, it is speculated that the high level of LHHCG may damage the endometrial receptivity and thus affect pregnancy outcomes. However, in our study, there was no significant difference in progesterone level on HCG trigger day between LHHCG < 2.58 IU/L group and LHHCG ≥ 2.58 IU/L group, which suggests that progesterone-mediated endometrial receptivity may not be the direct cause of the effect of LH level on pregnancy outcomes, and the specific mechanism needs further study.
The POSEIDON criteria further stratified the patients with poor or suboptimal ovarian response based on the Bologna standard. The female age in the ART cycle is related to the embryo aneuploidy rate and also be a sign of oocyte quality in the POSEIDON criteria [3]. Therefore, in this study the patients were divided into two groups according to age according the POSEIDON criteria, and we found that LHHCG level had a more significant predictive value for clinical pregnancy in advanced-aged women. Compared to the LHHCG ≥ 3.14 IU/L group, patients in the LHHCG < 3.14 IU/L group had higher HCG positive rate, embryo implantation rate, and clinical pregnancy rate. This is consistent with the study by Gao et al., which showed that among advanced-aged patients (≥ 37 years), the cumulative live birth rate in the group with abnormally elevated LHHCG was lower than normal LHHCG group [30]. Erhan et al. found that the high level of LH in the late follicular phase leads to early luteinization of oocytes and premature maturity of the endometrium, which leads to an abnormal implantation environment, especially in the advanced-aged women [31]. This may be one of the reasons why LHHCG is more significant in advanced-aged women and the pregnancy outcome in the group with high LH levels is poor in our study.
This was the first study to explore the predictive value of LHHCG in pregnancy outcomes in DOR patients in IVF/ICSI, and we found that LHHCG was an independent factor affecting clinical pregnancy rate in advanced-aged patients with DOR. Moreover, our results showed that high LHHCG level in the antagonist regimen was not conducive to the pregnancy outcome of the fresh embryo transfer cycle in patients with DOR, which suggests that we need to focus on LHHCG to comprehensively consider the feasibility of fresh embryo transfer.
Limitation
The main limitation of our study is that this is a retrospective study with inevitable selective bias. In addition, the sample size is limit, large-sample prospective trials and multicenter randomized controlled trials are still needed for further verification and clarify the specific mechanisms in the future.









留言 (0)