
記住我

This randomized controlled trial (RCT) took place at the Assisted Reproduction Centre of Northwest Women’s and Children’s Hospital, China, from March 2019 to January 2020. Women undergoing IVF/ICSI cycles were invited to participate in the study. Inclusion criteria were as follows: age < 40 years, utilization of the agonist long protocol, fresh cycle embryo transfer, and a serum estradiol level decrease of > 60% from the hCG trigger day to 3 days after oocyte retrieval. Exclusion criteria included an endometrial thickness < 8 mm, uterine malformation, endometriosis, and a peak serum estradiol level ≥ 5000pg/ml. All patients provided informed consent, and the study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Northwest Women’s and Children’s Hospital. Additionally, the study was registered in the Chinese Clinical Trial Registry under Registration No. ChiCTR1800020342. Reporting of the study adhered to CONSORT guidelines.
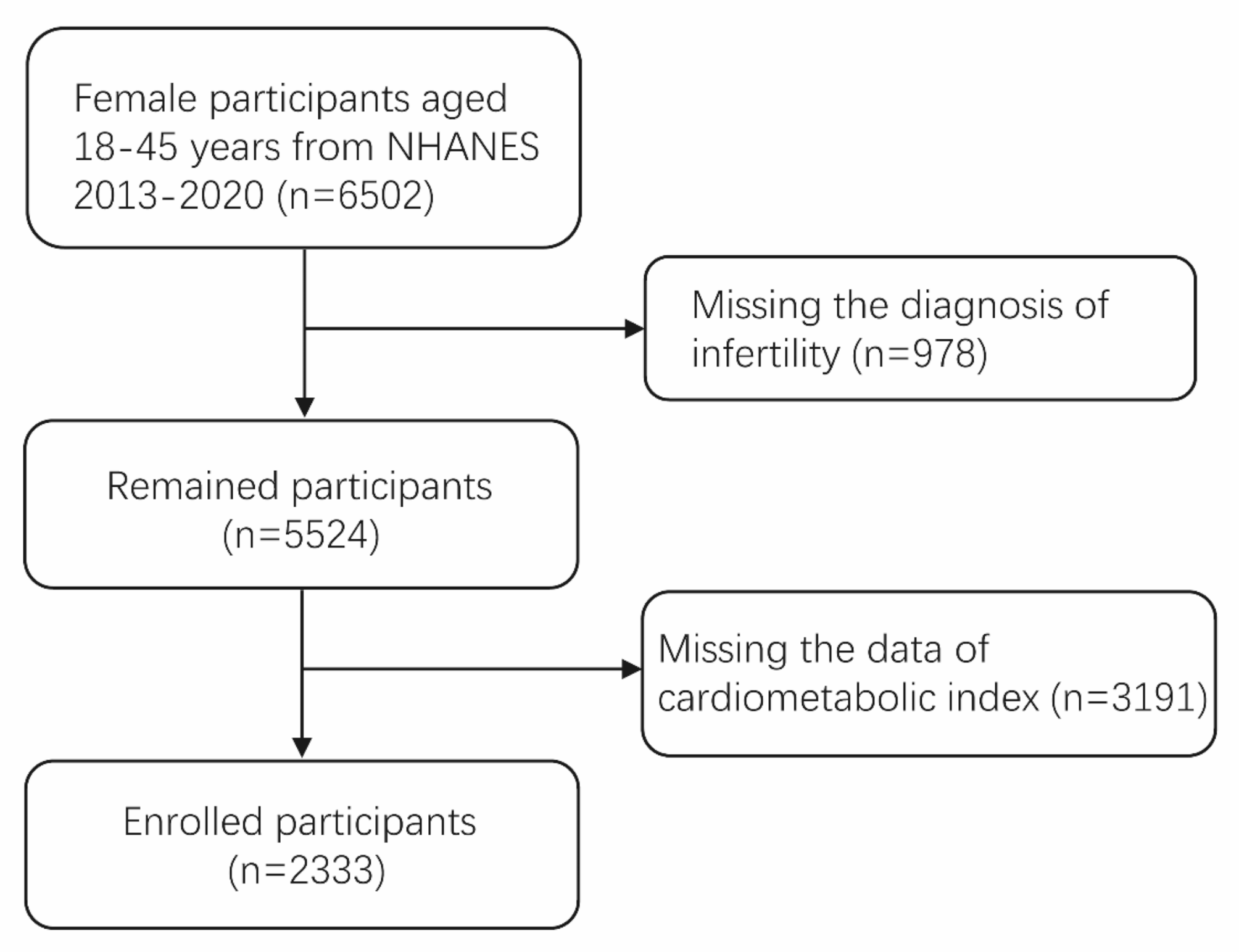
The flow of participants is illustrated in Fig. 1. Initially, a total of 1160 patients were considered for recruitment, but 915 were excluded due to not meeting the inclusion criteria (estradiol decline rate < 60%). In the final analysis, 20.68% of the screened patients exhibited an estradiol decline rate ≥ 60%. Four patients declined to participate, and 26 patients who consented were not randomized due to reasons such as unavailability of embryos for embryo transfer, risk of ovarian hyperstimulation syndrome (OHSS), or other factors. Ultimately, 219 patients completed the full allocated intervention and were randomized into the study group (E2 group, n = 106) and the control group (Control group, n = 113).
Fig. 1 Stimulation regimen
Stimulation regimenAll participants followed the agonist-long protocols, followed by the in-vitro fertilization/intracytoplasmic sperm injection-embryo transfer (IVF/ICSI-ET) regimen.
For those undergoing the long-term agonist protocol, subcutaneous administration of 0.1 mg triptorelin acetate (Decapeptyl, Ferring Ltd., Wittland, Germany) began in the mid-luteal phase of the preceding menstrual cycle and continued for 14 days.
After undergoing a baseline ultrasound scan, patients were deemed to have achieved a fully downregulated state when the following criteria were met: serum estradiol (E2) levels were below 50 pg/ml, luteinising hormone (LH) levels were less than 5 IU/ml, the endometrial thickness was less than 5 mm, and the diameter of the largest follicle fell within the range of 5–10 mm.
After achieving downregulation, recombinant follicle-stimulating hormone (rFSH, Gonal-F, Merck) was administered at a dosage ranging from 150 to 225 IU per day. When more than two follicles reached a diameter exceeding 18 mm, an injection of 6,500 to 10,000 units of Human Chorionic Gonadotropin (hCG) (brands such as Ovidrel, Merck; or Livzon) was administered.
Oocytes were retrieved via transvaginal ultrasound-guided follicular aspiration 36 h post-hCG injection, and the number of retrieved oocytes was recorded.
Blood samples and hormone measurementsBlood tests were conducted in the morning from 7:30 to 9:30. We routinely measure serum E2 levels on the day of hCG trigger, and in this study, we re-measured serum E2 levels on the third day after oocyte retrieval (as shown in Fig. 2), calculating the decline in E2 levels after retrieval by the difference between the latter and the former. Serum E2 concentrations were measured using an electrochemiluminescence immunoassay kit (Beckman Coulter, USA), with a minimum detection limit of 15 pg/mL. The intra- and inter-assay coefficients of variation were 4.3% and 5.5% for the low control and 5.1% and 7% for the high control, respectively.
Fig. 2
Research technical route. Ovum Pick Up (OPU), Blood draw for serum estradiol testing: (E2 test)
IVF/ICSI-ETOocytes were retrieved and fertilized using either the conventional method or intracytoplasmic sperm injection, depending on sperm quality. One to two embryos with the highest quality were selected for transfer on day 3 or 5. If more than two good quality embryos were available, they were cultured to the blastocyst stage, and single blastocyst transfer was preferred.
Randomization ProcedureRandom numbers were generated using a computer in a 1:1 ratio, and these numbers were then sealed in opaque envelopes. A postgraduate student, who was not involved in clinical work and was unaware of patient details, was tasked with grouping the patients randomly. Randomization occurred on the 3rd day after oocyte retrieval. Patients in both the trial and control groups were informed of their group assignments, which were also noted by clinicians. However, the embryologists and statisticians remained blinded to the group allocations.
Sample size calculationAccording to the optimization scheme, to achieve a 15% increase in the clinical pregnancy rate with 80% power and α set at 0.05, a sample size of 150 was determined for each group. Participant dropouts at baseline were not accounted for, with the reliability of the center’s follow-up system being the main consideration.
Luteal phase supportSerum estradiol levels were assessed in all enrolled patients on the hCG trigger day and 3 days after ovum pick up (OPU). If the E2 drop rate [(E2 level of OPU+ 3 day – E2 level of hCG trigger day)/ E2 level of hCG trigger day ×100%] exceeded 60%, patients were randomly assigned to two groups. The control group received conventional corpus luteum support, including progesterone injection at 60 mg/d intramuscularly, along with dydrogesterone at 20 mg/d orally or Crinone vaginal gel at 90 mg/d combined with dydrogesterone at 20 mg/d orally. In addition to conventional luteal support treatment, the study group (E2 group) received estradiol valerate at 4 mg/d orally from the 3rd day after OPU until the day of the serum beta-HCG test. Serum beta-HCG concentration was tested 14 days after ET. If pregnancy was confirmed, the progestogen was continued, and the estradiol dose was reduced by 1/3 every 3 days until discontinuation. Progesterone was continued in pregnant patients until approximately 10 weeks’ gestation to support the luteal phase.
Outcome measuresThe primary outcome measure was the ongoing pregnancy rate, while secondary outcome measures included the implantation rate, early abortion rate, clinical pregnancy rate, live birth rate, and the incidence of severe OHSS.
Outcome variablesBiochemical pregnancy: Serum beta-hCG level > 25mIU/ml.
Biochemical miscarriage: Positive pregnancy test without ultrasound evidence of a gestational sac.
Clinical pregnancy: Positive serum beta-hCG test result with ultrasound evidence of a gestational sac and fetal heart.
Implantation rate: Number of gestational sacs with fetal hearts assessed by ultrasound at 6–7 weeks’ gestation divided by the number of embryos transferred.
Ongoing pregnancy: Pregnancy progressing beyond 12 weeks’ gestation.
First-trimester pregnancy loss: Miscarriage after ultrasound evidence of an embryonic sac with or without a fetal pole not beyond 12 weeks.
Live birth: Birth of at least one newborn after 24 weeks’ gestation exhibiting any sign of life (twins counted as a single birth).
Statistical analysisData were analyzed using the statistical software packages R (The R Foundation; http://www.r-project.org; version 4.2.0) and EmpowerStats (www.empowerstats.net, X&Y Solutions, Inc. Boston, Massachusetts). Quantitative variables were presented as mean (standard deviation, SD), with the number of observations (N) provided. Categorical variables were expressed as number (percentage). The Kruskal-Wallis Rank Test was utilized for continuous variables, while Fisher’s Exact Test was applied for categorical variables with expected counts less than 10. The rate or mean difference between the groups, along with the 95% confidence interval (CI) and the corresponding P-value, were calculated using a Generalized Linear Model. A P-value < 0.05 was considered statistically significant.
留言 (0)