The Berlin long-term observation of vascular events (BeLOVE) study
The BeLOVE study is an ongoing long-term prospective observational cohort study of patients at very high risk for future cardiovascular events [24]. To meet inclusion criteria, patients must be at least 18 years of age and either recently hospitalized for an acute cardiovascular event (CVE) (acute coronary syndrome, acute heart failure, acute cerebrovascular disorder, and acute kidney injury) or at very high risk chronic cardiovascular conditions without event in the past 12 months. Pregnancy or breastfeeding, lack of health insurance, and life expectancy of ≤ 6 months due to a non-cardiovascular cause, active cancer, or a history of organ transplantation at the time of inclusion were defined as exclusion criteria. Moreover, patients unable to provide written informed consent are not considered for participation. Recruitment started in 2017 at the clinical campuses of the Charité - Universitätsmedizin Berlin and is ongoing.
The aim of BeLOVE is to improve prediction and understanding of disease progression and outcomes in patients with a very high risk of cardiovascular events, both in the acute and chronic phase, to ultimately improve and further personalize disease management. Assessments include comprehensive deep clinical and molecular phenotyping as well as ascertainment of clinical outcomes, e.g. major adverse CVEs, at predefined visits for up to 10 years.
In addition to clinical parameters, patient-reported outcome measures, including the PROMIS-29 profile and the SF-36, are administered at several assessment points of the BeLOVE study. Study data are collected and managed using REDCap [25, 26]. The present study utilized data from patients who were recruited during the first study phase of BeLOVE between July 2017 and December 2020 and had participated in the PROM collection part of the study.
MeasuresSF-36 physical (PCS) and mental (MCS) component summary scores
The SF-36 consists of eight domains: physical functioning (PF, 10 items), role function physical (RP, 4 items), bodily pain (BP, 2 items), general health (GH, 5 items), vitality (VT, 4 items), social functioning (SF, 2 items), role function emotional (RE, 3 items), and mental health (MH, 5 items) [14]. Scores of each domain can be transformed to a 0-100 scale.
The domain scores can be aggregated to physical (PCS) and mental (MCS) component summary scores; higher scores are representing better physical or mental health [16]. A norm-based T-score metric is used for scoring both the PCS and the MCS, with a mean of 50 and a standard deviation (SD) of 10 in the U.S. general population [16]. SF-36 PCS and MCS scores were originally derived using an orthogonal factor model, ‘forcing’ physical and mental components to be uncorrelated [16]. Since this original approach leads to potential problems with interpretation of results [17,18,19], modified scoring algorithms for correlated, i.e., oblique, SF-36 component summary scores (PCSc and MCSc), have been developed [20]. In the present study, we used component summary scores from both the orthogonal and the oblique factor solution, based on the German version of the standard SF-36 instrument with original recall periods (‘the past 4 weeks’ for most items) [16, 27].
The PROMIS-29 v2.0 profile
The PROMIS initiative, which was funded by the U.S. National Institutes of Health, developed item banks for many physical and psychosocial self-reported health domains [23]. All items of a given item bank are calibrated to a unidimensional T-score metric with a general population mean of 50 and a SD of 10, using IRT modeling [28]. A main advantage of IRT-calibrated item banks is that any item subset (e.g., short form) can be used to yield T-scores on a standardized scale [29, 30]. The PROMIS-29 v2.0 profile consists of 4-item short forms of seven HRQL domains (pain interference, fatigue, depression, anxiety, sleep disturbance, physical function, and ability to participate in social roles) and an additional single item measuring pain intensity on a 0–10 numeric rating scale [10, 21].
Analogous to the SF-36, the domains of the PROMIS-29 can be aggregated to physical and mental health summary scores, which are based on a correlated factor solution [21]; higher scores indicate better health. Many PROMIS measures have been translated into other languages, including German [31,32,33]. This study used the German version of the PROMIS-29 v2.0 profile [31].
Study samples
Within the BeLOVE study, both the PROMIS-29 and the SF-36 were performed during the deep phenotyping visits ~ 90 days (visit 3, V3) and two years (visit 6, V6) after the qualifying CVE for the acute disease entities or following study inclusion in the chronic CV arm in the BeLOVE Unit of the Berlin Institute of Health at Charité - Universitätsmedizin Berlin. Because most SF-36 and PROMIS-29 domains consists of few items and to ensure stable estimates, data from participants who did not answer all items of both measures were excluded for further analysis; this approach has been applied before [20]. In the present study, we used V3 data to establish algorithms to predict SF-36 summary scores from PROMIS-29 (‘calibration sample’), while V6 data were used to validate these algorithms (‘validation sample’).
Sample size considerations
With regard to the calibration sample, a minimum sample size of 509 was calculated to be sufficient for detecting a small effect (f2 > 0.02) in a linear regression model with eight predictors (power = 0.80, significance level = 0.05). A minimum sample size of 180 in the validation sample was calculated for detecting small effect sizes, defined as a standardized mean difference (SMD) of > 0.20 (power = 0.80, significance level = 0.05).
Statistical analysis
Based on data from the calibration sample, we fitted four separate linear regression models each for predicting SF-36 physical and SF-36 mental component scores [34]. These regression models differed by both the dependent variables (uncorrelated versus correlated SF-36 component summary scores) and the predictors (PROMIS-29 domain scores versus PROMIS-29 physical/mental summary scores).
For each model, assumptions of (multiple) linear regression analysis were checked [34]. We inspected partial regression plots to rule out non-linear relationships between dependent and independent variables. To identify outliers potentially biasing the regression model, we calculated Cook’s distance values (cut-off < 1). To test the assumption of independent residuals, we used the Durbin-Watson statistic [35], which should be close to a value of 2. Homoscedasticity was checked graphically [36]. Variance Inflation Factors were calculated to rule out multicollinearity in those models with multiple predictors (cut-off < 10).
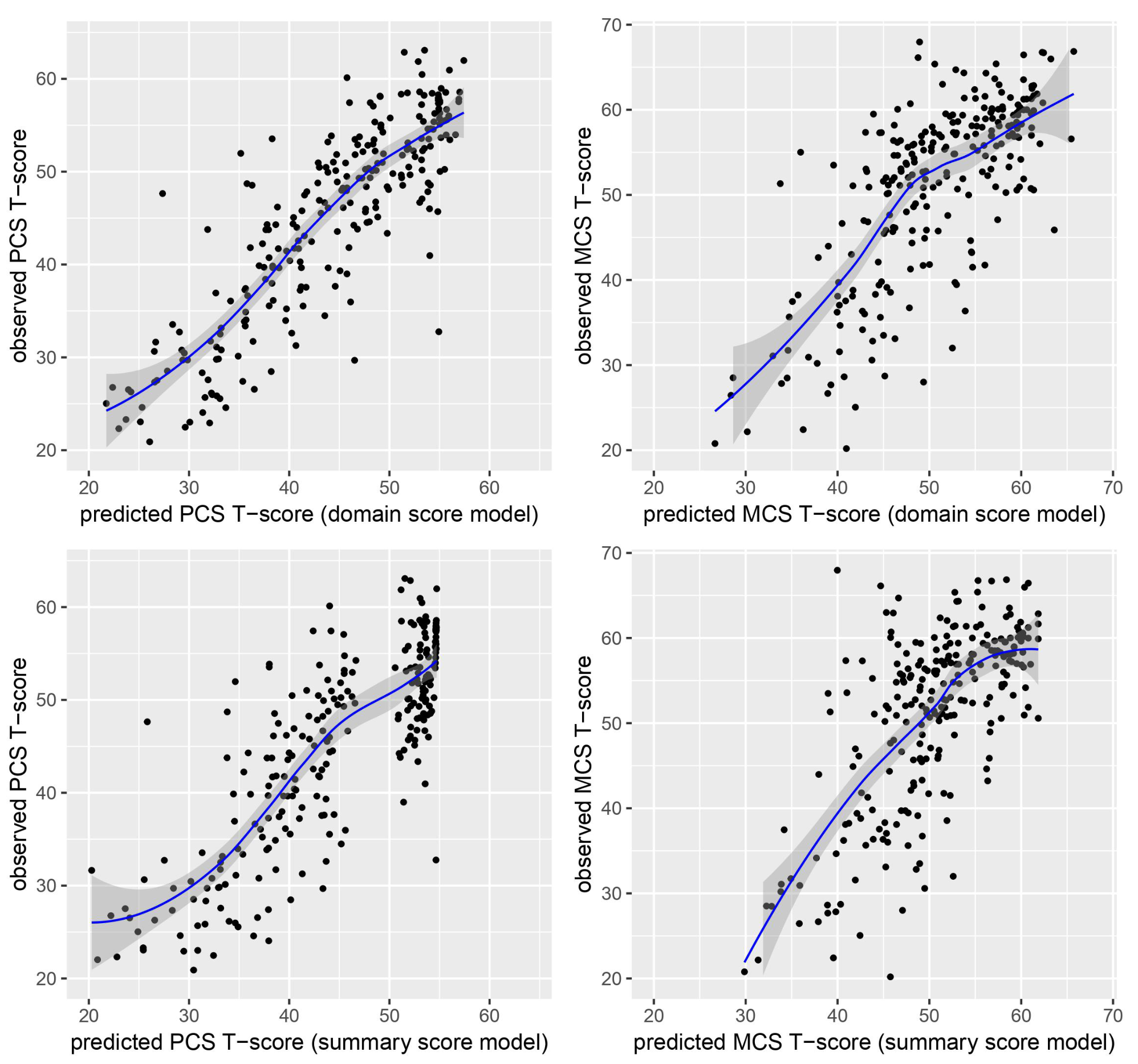
We then applied the established regression coefficients to predict SF-36 physical and mental component summary scores from PROMIS-29 data in the validation sample. Pearson correlation coefficients (r) were calculated to determine the association between empirical (i.e., ‘observed’) and predicted SF-36 summary scores. For calculating SMDs for paired samples, we utilized a pragmatic approach as described by Cumming (2012), which is appropriate for determining within-group effect sizes [37]. Specifically, we used the formula: SMD = mean difference between both measurements divided by the averaged standard deviation [37]. We considered SMD values of 0.2, 0.5, and 0.8 as small, medium, and large effects, respectively; values below 0.2 were considered negligible [38]. Mean absolute errors (mae), and root mean square errors (rmse) were used to compare the agreement between empirical and predicted scores across the different regression models [39, 40]. Smaller rmse and mae values indicate better agreement between empirical and predicted scores. Typically, the rmse is larger than the mae due to its sensitivity to larger errors.
For statistical analyses, R version 4.2.1 and the R packages ‘Metrics’, ‘effize’ and ‘pwr’ were used [40,41,42,43].

留言 (0)