
記住我





Eighteen well-trained male BJJ athletes (aged 32 ± 7.3 years; body mass 73.8 ± 10.8 kg; 174.9 ± 5.5 cm) with 8.9 ± 4.2 years of competition at international and/or national events completed this study.
The study was approved by the Ethics Committee of the Faculdade de Motricidade Humana, Universidade de Lisboa (CEIFMH—nr. 42/2021). The volunteers signed an informed consent, filled out a health questionnaire (Physical Activity Readiness Questionnaire, PAR-Q & YOU), and had their arterial blood pressure measured (Hartmann Veroval®, Heidenheim, Germany). Exclusion criteria included: (1) report of any cardiorespiratory or cardiovascular known disease; (2) any affirmative answer from the written PAR-Q & YOU; or (3) a systolic pressure above 140 mm/Hg and a diastolic pressure above 90 mm/Hg (American College of Sports Medicine 2018).
Experimental designThis was an experimental study with a randomized crossover design. Each athlete participated in three exercise sessions: a preliminary session where participants performed a maximal graded exercise test to assess peak oxygen consumption (\(}}\)O2peak) and familiarized themselves with the testing procedures and the VHL technique, and two other exercise sessions for RS evaluation, one using RSN and the other using RS-VHL. The RS sessions were randomly assigned and separated by at least 48 h within 15 days (Woorons et al. 2017). Participants were asked to avoid vigorous exercise, alcohol drinking, and caffeine 24 h before every test session and to maintain their regular diet throughout the study. All test sessions were performed approximately at the same time of day (±2 h) to avoid any potential effects of chronobiological variability on physiological responses (Pullinger et al. 2020; Fig. 1).
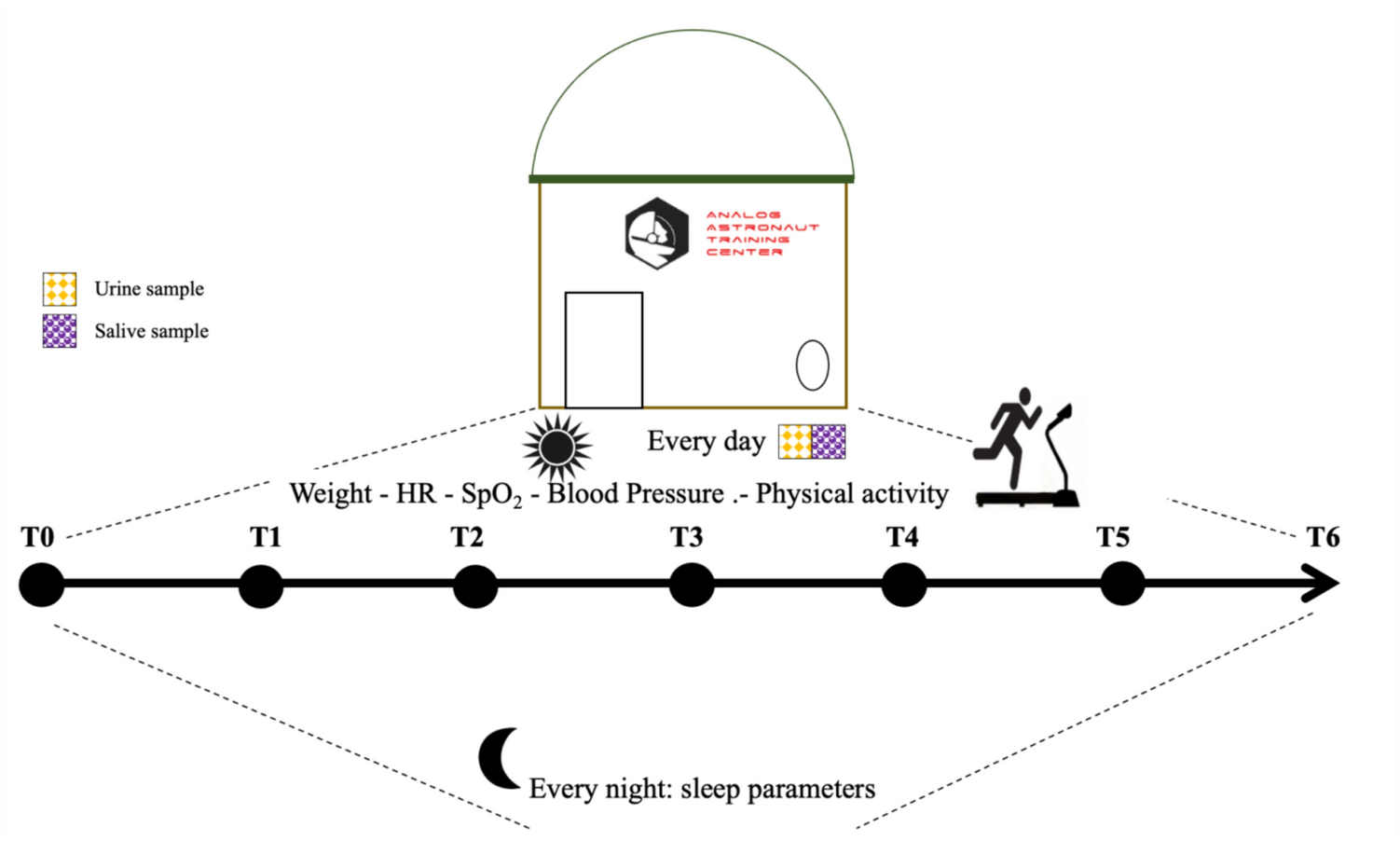
Fig. 1
Experimental design overview of the repeated sprints sessions
In the RS evaluation sessions, performance indicators, pulmonary gas exchange, heart rate (HR), arterial oxygen saturation (SpO2), and muscle oxygenation of the triceps brachii were evaluated during the RS protocols, and neuromuscular fatigue was assessed by measuring BPPP before and after the RS protocols. Rating of perceived exertion (RPE) and [La] were recorded during and at the end of the RS protocols. All the tests were performed on an arm-crank ergometer (Lode Angio, Groningen, The Netherlands). The configuration for each participant was replicated in every session. Participants remained seated with their shoulder joint aligned with the pedal crank axle.
Familiarization with the VHL techniqueTo familiarize the athletes with the VHL technique while arm-pedaling with no additional load (0 W), participants were asked to perform an end-expiratory breath-hold and to keep it until the first sign or urge to breathe; this exercise was then interspersed by long and deep unforced breaths. This was performed while controlling each inhalation and exhalation, for about 5 min. For the next 5 min, participants were asked to do the same procedure but to go further toward their limit while keeping the end-expiratory breath-hold and accelerating the pedaling rhythm during the breath holds. After these exercises, all subjects participated in four 6-s all-out sprints with 24-s passive rest while using VHL technique, simulating the experimental protocol.
Peak oxygen uptakeTo assess the \(}}\)O2peak, participants performed a maximal graded exercise test using an arm-crank ergometer. The protocol began with a 3-min warm-up with no load (0 W). After that, a load of 15 W was applied and increased by 15 W increments every minute until volitional exhaustion was attained (Antunes et al. 2022). Throughout the test, the participants were required to maintain a cadence of 70 ± 5 rpm (Price et al. 2007). All participants were given strong verbal encouragement during the test and were asked to remain seated to diminish any compensatory torso movements.
During the whole protocol, pulmonary gas exchange (\(}}\)O2, carbon dioxide, and respiratory exchange ratio, \(}}\)CO2, RER, respectively), ventilation (\(}}\)E), and HR data were continuously monitored. The \(}}\)O2peak was calculated as the highest 30-s \(}}\)O2 average attained during the protocol (Antunes et al. 2022).
Repeated-sprint protocolBefore starting the protocol, subjects performed a 5-min warm-up at low-intensity pedaling in the arm crank with no additional load while maintaining a cadence of 70 ± 5 rpm. Afterward, torque was set as the result of body weight times the distance between the midpoint of the pedal and the crank axle, as specified by the manufacturer, and a single 6-s all-out sprint was performed. The peak power output (PPO) was recorded to serve as a reference for the first sprint of the RS test protocol.
Testing began after a 5-min period of rest. The RS test protocol consisted of two sets (set 1 and set 2) of eight “all-out” 6-s sprints on the arm cycle ergometer. The 6-s sprints were separated by 24-s of passive recovery and 3 min of passive rest between the two sets (Woorons et al. 2017). In the first sprint of set 1, subjects were expected to achieve at least 90% of the PPO reached in the single sprint performed prior to the 5-min resting period. If this was not achieved, they restarted the set after a new 5-min period of rest (Woorons et al. 2017; Willis et al. 2019a, b).
Participants were strongly encouraged verbally and instructed to remain seated during RS protocol. To ensure the correct application of the VHL technique throughout the entire protocol, all participants were notified 5 s before the start of each sprint, and 2 s before the start, they were given specific instructions to exhale and hold their breath. Throughout both RS protocols, PPO, mean power output (MPO) and total work (TW), pulmonary gas exchange (\(}}\)O2, \(}}\)CO2, RER), \(}}\)E, HR, SpO2, and muscle oxygenation (oxyhemoglobin, deoxyhemoglobin, and tissue oxygenation index, respectively, O2Hb, HHb, and TOI) of the triceps brachii data were continuously monitored.
MeasurementsParticipants’ characterizationDuring the familiarization session, participants body mass (Seca, Model 761, Hamburg, Germany) and stature were measured (Harpenden, Holtain Ltd, Crosswell, UK) to the nearest 1.0 kg and 0.1 cm, respectively. Handgrip isometric strength (HGIso) of the dominant hand was also measured twice, separated by 1 min rest. Participants were asked to stand with the dominant arm extended along the trunk and to squeeze the dynamometer (Jamar, Lafayette, CA, USA) with the greatest possible force for 3–5 s. The highest value of the two repetitions was recorded.
PerformanceThe PPO and MPO were calculated for each of the 6-s sprints and TW was calculated as the result of the averaged power obtained in each of the 6-s sprints times the duration of the sprint (6-s).
Fatigue in each set was evaluated by calculating repeated-sprint percentage decrement score (RSAdecs) as follows:
$$} = (100 \times (}\,}\,}/}\,}\,}\,}\,}))--100,$$
where Sum of MPO = sum of MPO from all sprints of the set, and Ideal MPO of the set = highest MPO from all the sprints of the set × number of sprints of the set (Woorons et al. 2017).
Arterial oxygen saturationThe SpO2 was continuously measured during the RS protocols using a pulse oximeter placed on the ear lobe (Nonin PureSAT® SpO2 technology, WristOx2 3150 USB, Plymouth, USA), which was taped to diminish possible light interference and to ensure that the sensor was fixed throughout the protocol. Data were obtained once per second and averaged and analysed over 6 s. To account for the delay observed in the drop of the values, the lowest value obtained during or just after each sprint was used for further analysis (Woorons et al. 2017).
Gas exchange and heart rateThroughout the whole RS protocols, \(}}\)E, \(}}\)O2, and \(}}\)CO2 were collected breath-by-breath with a gas analyzer (MetaMax 3Br2, Cortex Biophysik, Leipzig, Germany) after calibration according to the manufacturer’s instructions. The HR was continuously recorded and monitored using an HR sensor (Polar® H10, Kempele, Finland). To account for the absence of data during breath holdings in the RS-VHL protocol, for both protocols, \(}}\)E, \(}}\)O2, \(}}\)CO2, RER, and HR data were analysed from the end of each sprint until the beginning of the next sprint and in the 24 s after the end of the last sprint of each set. Averages over 6 s were calculated, and the highest values of \(}}\)O2 (mL·kg−1·min−1), \(}}\)CO2 (L·min−1), \(}}\)E (L·min−1), RER, and HR (bpm) were used for analysis.
Muscle oxygenationThroughout the RS protocols, changes in O2Hb and HHb concentrations and TOI from baseline were measured by near-infrared spectroscopy (NIRS) (Niro 200, Hamamatsu, Japan). The skin was shaved and the NIRS probe was placed on the belly of the long head of the triceps brachii, because this muscle participates in both elbow and shoulder extension; an elastic non-compressive bandage was wrapped around the probe and arm to prevent movement of the probe and any potential source of light interference. A pen and photographic record were used to mark the probe placement for test replication. Basal tissue oxygenation values were obtained after 1 min at rest while sitting on the chair before warm-up in each condition. To attain for any possible delay in the response of muscle oxygenation variables, data were averaged over 6 s and analysed from the beginning of each sprint to the beginning of the next or to the 24th second after the end of the last sprint, in each set. The lowest values of O2Hb and TOI and the highest values of HHb in each sprint were kept for analysis.
Rating of perceived exertion and blood lactate concentrationIn both exercise conditions, RPE was obtained immediately after the end of each set using the Modified Borg Scale (range 0–10) (Woorons et al. 2017).
[La] were obtained using a Lactate Pro device (Arkray, Kyoto, Japan). A blood sample from the ear lobe was collected by capillary puncture 1.5 min after the end of both set 1 and set 2 and 3 min after the end of set 2. The highest value of the two samples collected at the end of set 2 was kept for analysis (Woorons et al. 2017).
Neuromuscular fatigueIn each RS session, before and after the RS protocol, the participants’ BPPP was measured to assess neuromuscular fatigue. Before the RS protocols, two sets of three throws were executed 1 min and 30 s apart, the first set (warm-up) with 25% and the second (main set) with 50% of the body weight. Only the main set was performed after the RS protocols. Chronojump Boscosystems® linear encoder and Chronojump software version 1.9.0 (Chronojump, Barcelona, Spain) were used to measure and record BPPP of each repetition, and the best repetitions of the main sets were kept for analysis.
Statistical analysisStatistical analysis was performed using IBM SPSS Statistics (Version 28.0, IBM, NY) and R software (Version 4.2.0, Open-Source Code, General Public License). Based on an effect size of 0.4 and power of 0.8, a priori power analysis (GPower Version 3.1.9.3) for two-way repeated-measures analysis of variance suggested a total of 14 participants. All the results are expressed as mean ± SD. The data were analysed using a general linear model for repeated-measures analysis of variance (ANOVA), considering the condition of O2 availability (RS-VHL or RSN), sets (set 1 and set 2), and sprints (from 1 to 8) as three within factors. Huynh–Felt correction was used to attain eventual violations of sphericity in the sprint factor. For RSAdecs, [La], and RPE, analysis of variance (ANOVA) was performed using a general linear model for repeated measures considering the condition of O2 availability (RS-VHL or RSN) and sets (set 1 and set 2) as two within factor. When an interaction between the within factors was observed, pairwise comparisons with Bonferroni adjustment were performed to assess simple main effects. If normal distribution was not verified, the nparLD module of the R software was used to perform a non-parametric two-way ANOVA-type test, and Wilcoxon signed-ranks tests were used to assess simple main effects and differences between conditions for complete protocols. Significance (p) was set at 0.05.
留言 (0)