Technical Assessment
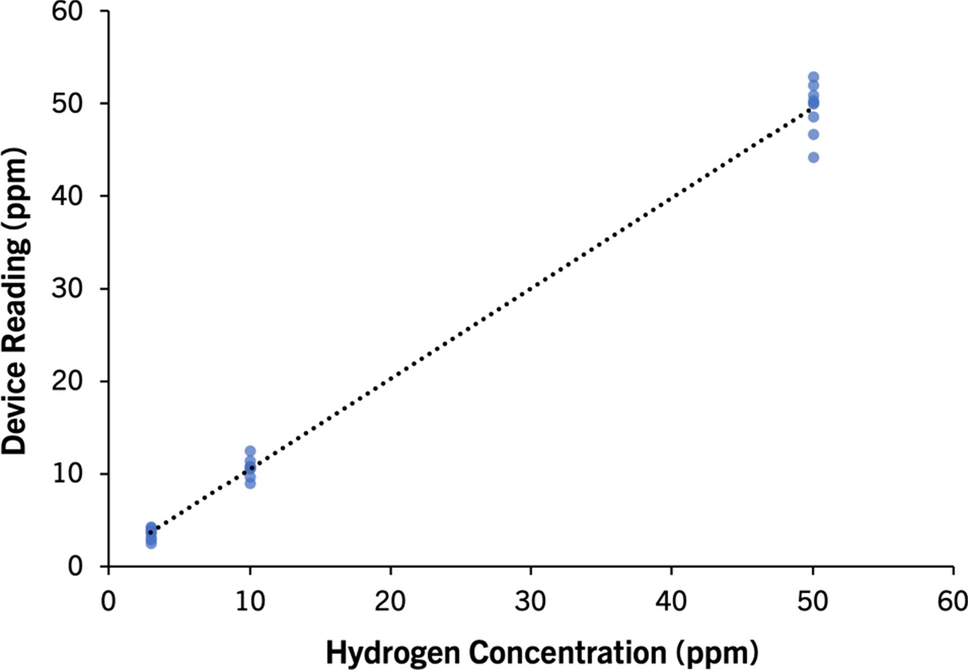
The technical performance and repeatability of the AIRE device were determined by an ISO 17025:2017 accredited testing and calibration laboratory (GAS Analysis Services, Wicklow, Ireland). Certified test gases (hydrogen mixed with air at 3, 10, and 50 ppm) were analyzed using a gas chromatography machine to verify their concentrations. The test gases were heated and humidified to replicate human breath (24 °C ≤ temperature ≤ 28 °C, 80% ≤ relative humidity ≤ 95%). The test gases were passed through each AIRE device for five seconds to match real world operation. Each device was tested three times using each test gas sequentially, with a 15-min gap between each test to replicate a typical LHBT testing scenario. Three AIRE devices were tested three times at each test gas concentration on three non-consecutive days.
Study Subjects
The study population consisted of adult patients suspected to have SIBO based on chronic (3 months or more) GI symptoms including nausea, bloating, distention, altered bowel movements, weight loss, or abdominal pain with no evidence of mechanical obstruction. Exclusion criteria included a history of inflammatory bowel disease or antibiotic use within 30 days prior to study commencement. The study was registered with ClinicalTrials.gov (NCT04309396).
Performance of LHBT
Subjects performed simultaneous LHBTs at-home using the AIRE device and a commercially available mail-in kit (Commonwealth Diagnostics International, Salem, MA, United States or Trio-smart, Raleigh, NC, United States). LHBTs were performed in a standardized manner using the instructions provided by each manufacturer. With Commonwealth Diagnostics International mail-in kits, subjects are instructed to exhale into a collection tube for 3–5 s. With Trio-smart mail-in kits, subjects are instructed to exhale into a mouthpiece attached to a collection bag for 2 s. A hole in the mouthpiece allows dead space air to escape. After 2 s, the subject covers this hole while continuing to exhale until the bag is filled (approximately 3 s). Mail-in kit samples are analyzed for carbon dioxide (CO2) concentration. An end-tidal breath sample is required for a reliable breath test result, which should contain approximately 5.5% CO2. In cases where the breath sample is contaminated by dead space or room air, due to improper collection technique, a correction factor is applied to the final breath result. With the AIRE device, the subject is instructed to hold their breath for 3 s before exhaling to allow for adequate gas exchange in the lungs. The FoodMarble app provides a countdown timer on screen to guide the patient. Upon exhalation, the subject is instructed to breathe slowly into the device for 5 s to ensure an end-tidal breath sample. If a subject stops breathing before 5 s have been reached, they are prompted by the FoodMarble app to retake the breath sample one minute later.
In line with the North American Consensus on breath testing in gastrointestinal disorders, a positive LHBT was defined as a ≥ 20 ppm rise in breath H2 above baseline within 90 min of substrate consumption [16]. Where breath test timings were not recorded at exactly 90 min post substrate consumption for either device, data were linearly interpolated. Subjects were required to follow a diet low in fermentable carbohydrates for the 24 h before the test. They underwent a minimum of 12 h fasting, where only water was permitted. On the morning of the LHBT, subjects checked their fasting breath H2 levels using the AIRE device and app. If their fasting breath H2 was elevated (> 15 ppm), they were advised to re-check it in 20 min intervals for up to one hour. If their fasting breath H2 remained elevated, they were advised to postpone the test until the following morning. A baseline breath reading was recorded on the AIRE device and using the mail-in kit. The test substrate, 15 mL of lactulose, was ingested. Every 15 min a breath test was recorded on the AIRE device and the mail-in kit for a minimum of two hours. Upon completion of the LHBT, the FoodMarble app automatically confirmed adherence to the LHBT protocol and notified the subject that test results had been sent to their healthcare provider for review via the FoodMarble online dashboard. The commercial LHBT kit was mailed by the subject to a testing lab for the measurement of the breath test samples. Results were received by PDF within 3–10 days.
Postprandial Breath H2 Measurement
Twenty four patients and 10 healthy controls were instructed to follow their habitual diet throughout the study. Both groups used the AIRE device and app to measure exhaled breath H2 content before and after the first (morning) and last (evening) meal of each day. Prior to eating, a baseline breath reading was recorded. After finishing each meal, a breath reading was recorded at 30, 60, and 90 min. Patients recorded breath data for 7 days prior to antibiotic treatment and for 7 days after completion of treatment. Post-treatment data were gathered 2 weeks after the completion of antibiotic therapy. A subset of patients (14/24) also recorded breath data during treatment. Healthy volunteers recorded breath data for 7 days.
Statistical Analysis
Postprandial breath H2 comparisons between groups were made using one-way analysis of variance (ANOVA). Subsequently, post hoc comparisons were conducted using the Bonferroni test to discern specific pairwise differences between groups. A p value ≤ 0.05 was considered statistically significant. This analysis was performed using IBM SPSS software version 28.
The sample size for the LHBT comparison was calculated using the methods of Buderer et al. [17]. For the calculation, a sensitivity of 42% and a specificity of 70% were used [18]. A target population prevalence of 36.7% was used [19]. Using these parameters, a sample size of at least n = 48 was defined for the LHBT comparison.
Correlations between breath H2 concentrations from the AIRE devices and mail-in kits were determined using Pearson’s correlation and simple linear regression analysis. This analysis was performed using IBM SPSS software version 28. A p value ≤ 0.05 was considered statistically significant. Mean and standard deviation of baseline, peak, and overall H2 concentrations were calculated. To assess diagnostic agreement, Cohen’s kappa statistic was also calculated. Mail-in kit LHBT reports may return individual breath test results as ‘invalid samples’ due to insufficient gas samples being present in the collection tube or bag at the time of analysis. Results that were reported as ‘invalid samples’ were omitted from the statistical analyses. All pairwise comparisons were made with viable samples from the AIRE device and the mail-in kit.


留言 (0)