This study aimed to quantify the preferences of a sample of GPs and pharmacists for the design of a pharmacogenetic testing service intended for primary care in the NHS. The findings show respondents preferred pharmacogenetic testing over no testing. However, both professional groups, and especially GPs, were highly sensitive to service design, with predicted uptake varying considerably depending on the service offered. No difference in preferences was identified based on the clinical scenario, though a difference was found based on professional role. This represents the first study to quantify the views of two professional groups, able to prescribe medicines, to inform the development of a pharmacogenetic service in primary care.
In both professional groups, respondents preferred to receive pharmacogenetic results via a “narrow” gene panel, rather than a “focussed” single result or a “broad” panel. With an average clinic appointment time of 10 min, it is understandable that GPs preferred results that were immediately actionable [21]. Any requirement to consider the level of evidence and actionability for individual genes and variants, as might be required with a “broad” panel, is unlikely to integrate into an already complex and time-sensitive environment [22].
Though pharmacists also preferred “narrow” results, they were not significantly opposed to receiving more detailed data. This may reflect their distinct role in leading the medicines optimisation process where there may be relatively greater scope to consider these less definitive findings. It may also reflect differences in training, with pharmacists potentially having more exposure to pharmacogenetics education during their undergraduate curricula [23]. Indeed, pharmacist-led medication reconciliation programmes, augmented by pharmacogenetics, have been successfully implemented into routine practice in other health systems [4, 24, 25]. This suggests there is space for a dual model of pharmacogenetic implementation in primary care, with pharmacists and GPs playing distinct but complementary roles.
Both professional groups strongly preferred services where results were returned directly within the EHR and, conversely, were more likely to reject services where results were returned via post or email. There are a range of different approaches to how pharmacogenetic data might be stored and surfaced within an EHR from basic solutions such as returning a portable document format file (PDF), to more advanced solutions such as creating clinical decision support (CDS) notifications [26, 27]. Prescribing support software tools are already commonly used in UK general practice to surface CDS alerts and prompts during the prescribing workflow based on patients test results, but these are not in place for pharmacogenetic data [28]. Any solution which necessitates messaging data across institutional boundaries, from laboratory to GP practice, will require the development of technical systems and data standards to facilitate interoperability and clinical interpretation [29]. Compared to other areas of the NHS, General Practice is significantly more advanced with respect to interoperable IT infrastructure, with long established links between practices and pathology departments [30, 31]. However, no comparable system exists for genomic data. These findings suggest that this should be addressed as a priority if pharmacogenetics is to be implemented in routine clinical practice.
These results show that the design of a pharmacogenetic service materially impact predicted uptake and is as relevant as the potential prescribing improvements offered by the test itself. The ability of a pharmacogenetic test to improve safety or improve effectiveness will vary depending on the clinical context, including the baseline risk without testing. The PREPARE study, an implementation trial of a “narrow” 12-gene pharmacogenetic panel across seven European countries, found a reduction of clinically relevant ADRs of up to 30% [6]. The findings from this DCE suggest that a reduction in ADRs alone is not sufficient to foster widespread uptake amongst both professional groups, but especially GPs. Delivering any pharmacogenetic intervention using current (“baseline”) infrastructure would result in imperfect uptake, something which should be reflected in any health-economic modelling, but has been neglected in many previous analyses [32, 33].
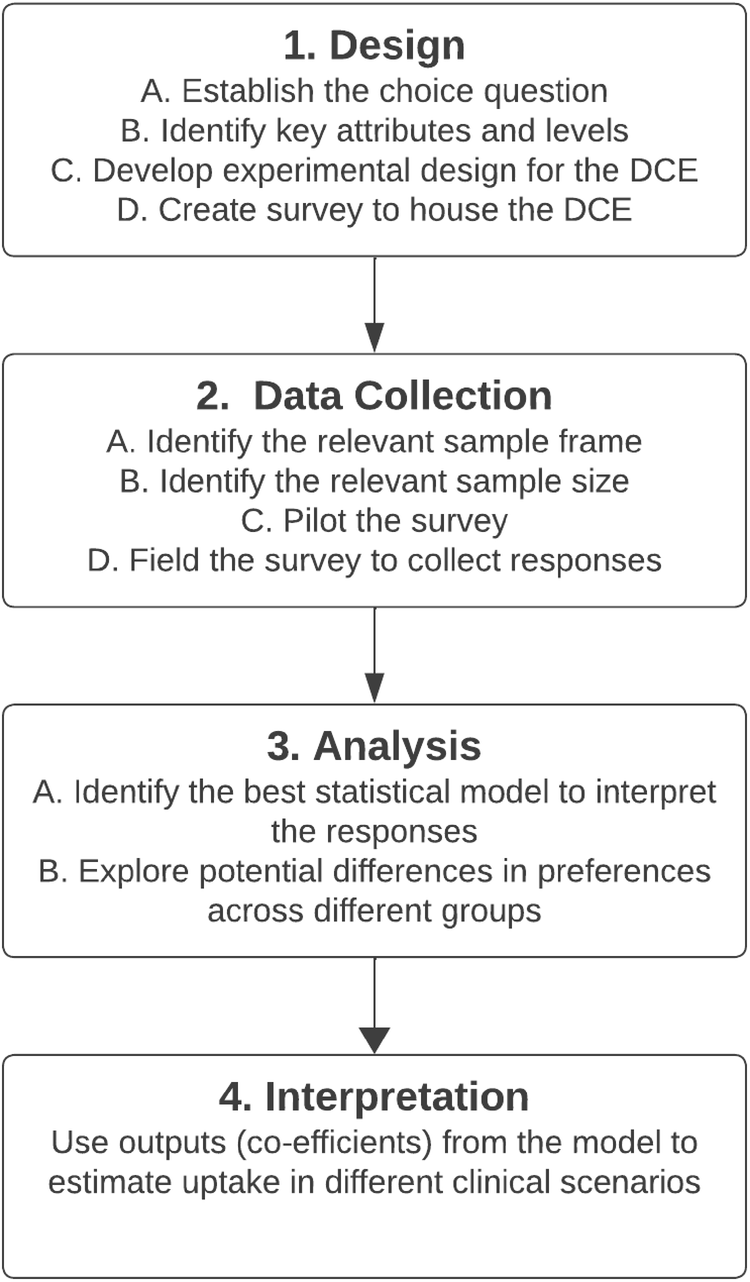
DCEs represent an approach to measure choices and infer stated preferences and, although estimates suggest they produce reliable predictions, they are susceptible to hypothetical bias [34]. Given current pressures experienced within primary care, even if an optimised service were developed, it is possible that pharmacogenetic testing might not be routinely requested when considered amongst the hierarchy of demands experienced by GPs and pharmacists on a daily basis. It should also be noted that any survey can be subject to sampling bias, and the stakeholders who completed the survey may not be fully representative of the primary care population as a whole with only those already interested in pharmacogenetics completing the survey. Additionally, these findings may not be generalisable to other healthcare professionals or healthcare settings, and independent replication would be required.
These findings highlight which aspects of a service might impact uptake, which can be used to guide design. However, stated preferences are unlikely to identically match revealed preferences, especially as other factors not tested here such as access to testing, reimbursement mechanisms, and availability of guidance are also likely to all influence uptake. As such, any changes made to services based on these findings should be tested in practice, using revealed preference methodologies, prior to wide-spread implementation.
There is a high level of acceptability for pharmacogenetic testing in primary care, but this is contingent on the service being designed appropriately. As such, implementation programmes should focus not only on making testing available but consider the full clinical pathway including digital and data interoperability. This will require dedicated resource and expertise, requiring the involvement of clinical stakeholders from the outset. The organisational challenges and financial investment to achieve this at scale will be substantial, but these findings suggest that the potential rewards are considerable.




留言 (0)