
記住我



This study was a community-based intervention study adopting a stepped-wedge cluster randomised design (SW-CRT) with islands as the cluster unit. It is well understood that the stepped-wedge cluster design is a type of crossover cluster trial where a cluster starts in the control condition and receives an intervention the later stage [22]. Given the high prevalence of S. mekongi identified in our baseline assessment on both islands (28.4% in the control group and 29.1% in the intervention group), the SW-CRT design is both beneficial and ethically sound since the interventions are being implemented equally across both islands.
We hypothesized that the Eco-Health/One-Health approach would significantly impact S. mekongi and other helminth infections of public health importance, such as O. viverrini, hookworm, and Trichuris trichiura, supplementing the conventional MDA approach. Primary study outcomes included the prevalence of S. mekongi infection, intensity of infection, and knowledge, attitudes, and practices related to its transmission. Secondary outcomes comprised the prevalence and intensity of O. viverrini, hookworm, and T. trichiura infections.
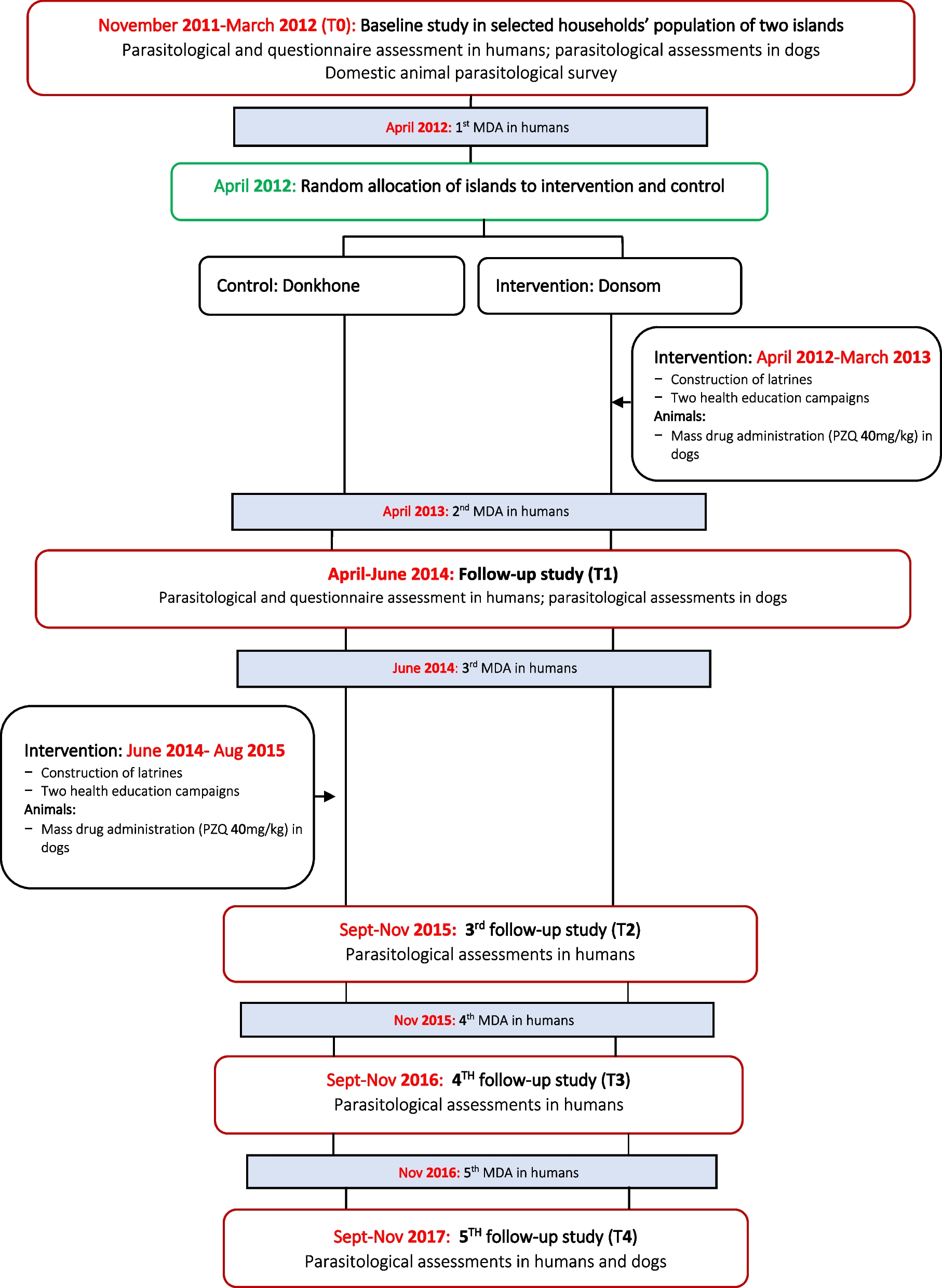
The trial was executed in two phases (Fig. 1) on the Donsom and Donkhone islands in Khong district, Champasack province, Southern Lao PDR, known as endemic islands for schistosomiasis and other helminthiasis such as O. viverrini, hookworm, and T. trichiura [2]. This phase 1 spanned from 2011 to 2014, during which the baseline (T0) was conducted to collect socio-economic data, knowledge, attitude, and practice towards schistosomiasis prevention and personal hygienic behaviour and the helminth infections in humans and animals on both islands. In each study village, about 30–40 households were randomly selected, and all members of these households aged 2 years and older present on the survey day were invited to participate in the study. In addition, all dogs owned by the selected households were also enrolled for parasitological assessment. Following this T0, two islands were randomly assigned to either the intervention (Donsom) or control (Donkhone) groups by the research team. The intervention group received the Eco-Health/One-Health approach in addition to the traditional MDA (one time per year), while the control group received only the MDA. One year after the completion of the intervention, the assessment study (T1) was conducted to evaluate the impact of the intervention compared to the baseline (T0). This follow-up assessment was carried out with the same individuals who were initially enrolled and had completed the baseline study.
Fig. 1
The phase 2 of the trial was initiated in 2015, with Eco-Health/One-Health approach implemented on the control island (Donkhone), and the parasitological assessment was conducted annually in 2015 (T2), in 2016 (T3), and in 2017 (T4) in humans. The same households (30‒40 per village) that were included at the initial time point (T0) continued to participate in these parasitological assessments throughout the project. However, the follow-up shifted from an individual-based to a household-based assessment. Members of the selected households who were aged 2 years and older and were present at home during the assessment were invited to participate in the study. On each island, we invited 350 participants to achieve our target sample size of 622 individuals. While in dogs the assessment was only done at the endline in 2017 (T4).
Study area and populationKhong district is one of ten districts in Champasack province, the biggest southern province of Lao PDR. This district has some 100,000 people and is located in the south of the province, at a distance of about 120 km from Pakse, the main city of Champasack province [23]. For this, two islands (Donsom and Donkhone) known as endemic areas for schistosomiasis in the Khong district were selected as the study setting [3]. Donsom has five villages with 378 houses and 2344 villagers, and three villages (Veunsom, Somven-tok, and Somven-ok) were enrolled in the study. Donkhone has three villages (Khone-neua, Khone-tai, and Hangkhone) with 260 houses and 1560 villagers and all three villages were enrolled.
Sample size calculationWe estimated that the prevalence of S. mekongi on the control island would remain unchanged at 30%, as detected by the Kato-Katz method. In contrast, on the intervention island, we projected a prevalence of 20%, resulting in a difference in prevalence of 10% after one year of follow-up assessment. We set the precision at 5% and aimed for a statistical power of 80%. We used a confidence level of 95% (a Z-alpha of 1.96 and a Z-beta of 0.84), and applied a design effect of 1.1 to account for the cluster design. Based on these parameters, we calculated the minimum required samples per island of 296 participants. Anticipating a 10% loss to follow-up in one year’s assessment the intervention, we adjusted the required sample size to 326 participants per island, or a total of 622 participants across both islands.
Development and implementation of intervention packageWe developed our Eco-Health/One-Health approach in consultation with key stakeholders in a workshop held on April 15, 2012, at the Khong district governor’s office. Representatives from the national, provincial, district, and community levels were invited and joined this workshop. In this workshop, the findings of the baseline assessment were presented and discussed. Thereafter, potential community interventions were proposed, and their adequacy, applicability, and acceptability were discussed. The following Eco-Health/One-Health approach was retained, consisting of three components. First, a comprehensive latrine construction programme promotes and encourages people to build and use latrines. Second, educate villagers about the target diseases and their prevention through effective health education. Third, the MDA with praziquantel (40 mg/kg) for all dogs in the study villages. In addition, a MDA in humans was conducted on both intervention and control islands, targeting all populations aged 4 years or older according to national guidelines [24, 25]. The treatment consisted of a single oral dose of praziquantel (40 mg/kg body weight) and a single oral dose of albendazole (400 mg).
The intervention was carried out by local institutions and communities. The construction of latrines on the study islands was the full responsibility of each household participating in the study, with minimal material subsidies provided by the project (e.g., toilet bowls, septic tanks, and metal roofs). The construction process was closely supervised by village authorities, with technical support from the Division of Environment Management and Water Supply of the Provincial Health Department in Champasack province. MDA in humans was performed by medical staff from the Provincial Station for Malariology, Parasitology, and Entomology of the Provincial Health Department, as well as the District Health Office. In the case of dogs, MDA was conducted by animal health personnel from the Provincial Department of Agriculture and Forestry, as well as the Khong District Office of Agriculture and Forestry in Champasack province and Khong district, respectively. Lastly, health education campaigns were conducted by the research team and medical officers from the Division of Hygiene and Health Promotion at the Provincial Health Department in Champasack province.
Questionnaire survey and parasitological proceduresWe employed two questionnaire forms to collect the epidemiological data and two standard parasitological methods such as Kato-Katz (KK) [26] and formalin-ethyl acetate concentration technique (FECT) [27, 28] to assess the helminth infections throughout the study periods (phase 1 and phase 2). Detailed questionnaire surveys and parasitological examination procedures were outlined by Vonghachack and colleagues (2017) [3]. In brief, a household questionnaire introduced to a head of each household. This questionnaire was designed to gather data on various aspects. These included the characteristics of the household, such as the type of house, toilet facilities, and water supply. It also covered the ownership of assets, including items like farm engines, boats, cars, motorbikes, electricity, televisions, bicycles, telephones, and agricultural land. Additionally, it included information on the types of animals owned by the household, such as buffaloes, cows, goats, pigs, cats, and dogs. Moreover, an individual questionnaire was applied to each member of the study household. This was designed to gather demographic information such as age, gender, level of education, and professional activities. It also collected data on knowledge about schistosomiasis, its transmission route, its endemic area, and personal behavioural risks, including food consumption habits, contact with water, animal rearing practices, and open defecation and hygiene practice. For children under the age of 10, their parents or legal guardians provided the necessary responses.
From each human participant, two stool samples were provided during baseline and all follow-up studies. Each stool, two Kato-Katz smears were prepared, resulting in a total of four smears, which were then examined by experienced laboratory technicians after 15 min of preparation. For each dog, two grammes of stool sample were collected and preserved in a 10% formalin solution. The preserved stool samples were transported to Lao TPHI’s laboratory in Vientiane, where they processed and analyzed by experienced laboratory technicians using FECT. All helminth eggs detected under the light microscope were counted and recorded separately for each helminth species. Quality control measures were implemented, involving a senior laboratory technician reviewing 10% of the reading slides. Any discrepancies found in slide readings were addressed through consensus findings among laboratory technicians.
Data management and analysisAll questionnaires and data forms were double-checked for completeness and consistency of the data by a senior researcher at the Lao TPHI before data entry. EpiData software, version 3.2 (Epi-Data Association; Odense, Denmark), was utilized for the data entry. Two data clerks were employed for a double data entry. The validation of data entry was performed to ensure accuracy and completeness. The cleaned dataset was exported to the STATA software, version 14, (Stata Corporation, College Station, United States) for statistical analysis.
The household’s socio-economic wealth index was constructed based on the household’s asset based approach, which was widely used, and details of the construction were previously described elsewhere [3, 4, 29]. The household’s socioeconomic status (SES) was classified into five wealth quintiles based on their cumulative standardised asset scores: (i) most poor, (ii) very poor, (iii) poor, (iv) less poor, and (v) richest. The age of participants was categorised into five groups: (i) ≤ 9 years, (ii) 10–17 years, (iii) 18–37 years, (iv) 38–49 years, and (v) ≥ 50 years. The impact of intervention on helminth infections associated with the intervention package was calculated using the percentage of the reduction in prevalence in the intervention group minus the percentage of the reduction in prevalence in the control group. The arithmetic mean with a 95% confidence interval was used to calculate egg counts per gramme of stool sample.
The coverage of each MDA was calculated using the number of targeted inhabitants who received the treatment divided by the total number of eligible inhabitants (aged 4 years and older) for MDA multiplied by 100 and stratified by setting. The χ2 test was performed to examine the different distribution of the baseline socio-demographic characteristics between the control and intervention groups. Logistic regression was applied to associate the KAP (knowledge, attitudes, and practices and open defecation behavior) and the reduction of helminth infections between intervention and control islands. The reduction in prevalence pre- and post-intervention was associated using a McNemar test. A two-independent sample t-test was applied to compare the mean eggs per gram (EPG) of helminth infections between control and intervention islands. A paired t-test test was used to compare the mean EPG of stool samples before (baseline) and after (follow-up) interventions for the two islands separately. A P-value lower than 0.05 was considered statistically significant.
留言 (0)