When patients have ACS VEMP testing and there is no response, it is unclear if this is due to the stimulus procedure, middle ear pathology, or a real vestibulopathy [13]. In various studies available in the literature, it has been shown that the obtainability of VEMP responses decreases with AC stimuli in conductive hearing loss [13, 14]. For this reason, studies have been directed towards the use of BC stimuli in conductive hearing loss.
There are articles in the literature comparing the results of tendon hammer tap, Radioear B-71 and mini-shaker [13]. Iwasaki et al. (2008) compared mini-shaker and Radioear B-71 in BC oVEMP and reported that B-71 did not provide sufficient stimulation [15]. However, since different transducers will not be available in every clinic, we aimed to obtain bone tract responses with a different stimulus.
Curthoys et al. (2010) reported that the position of the bone oscillator on the skull may also influence the results [6]. Therefore, in our study, we switched between stimuli without changing the location of the oscillator. The fact that we were able to get a response with Chirp stimulus in participants who could not respond with TB stimulus made us conclude that Chirp stimulus is a better stimulus than TB stimulus in BC cVEMP.
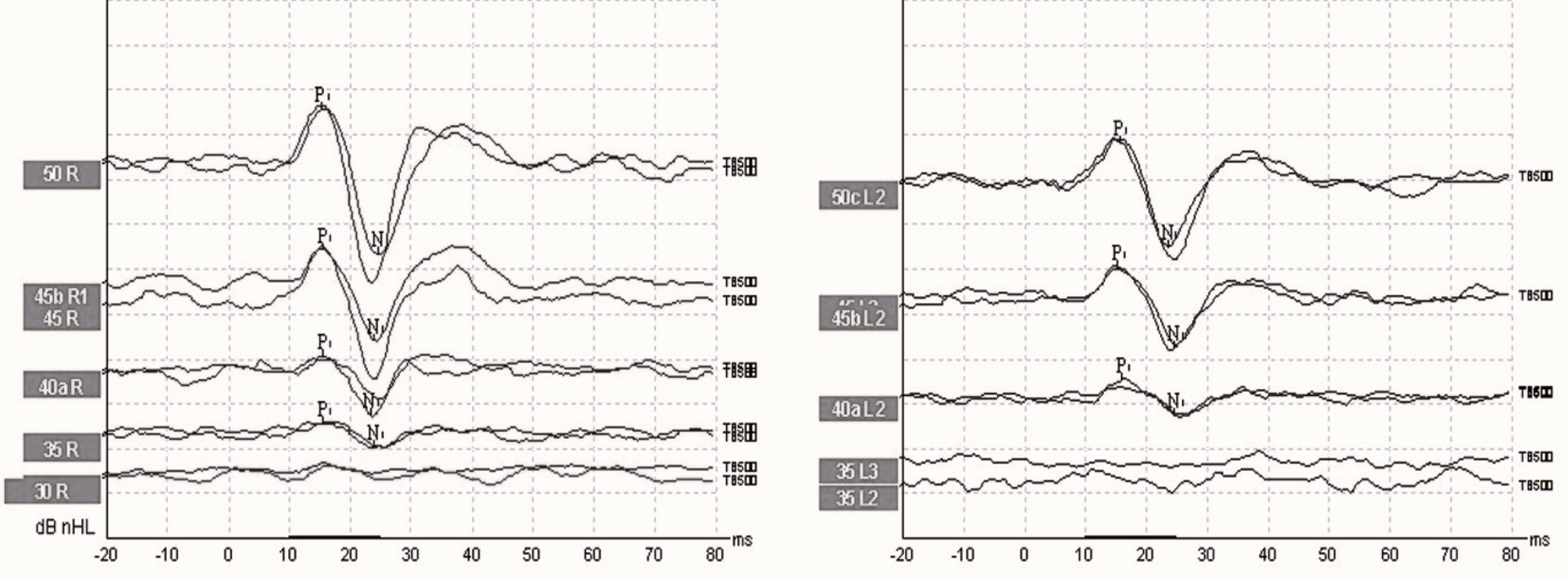
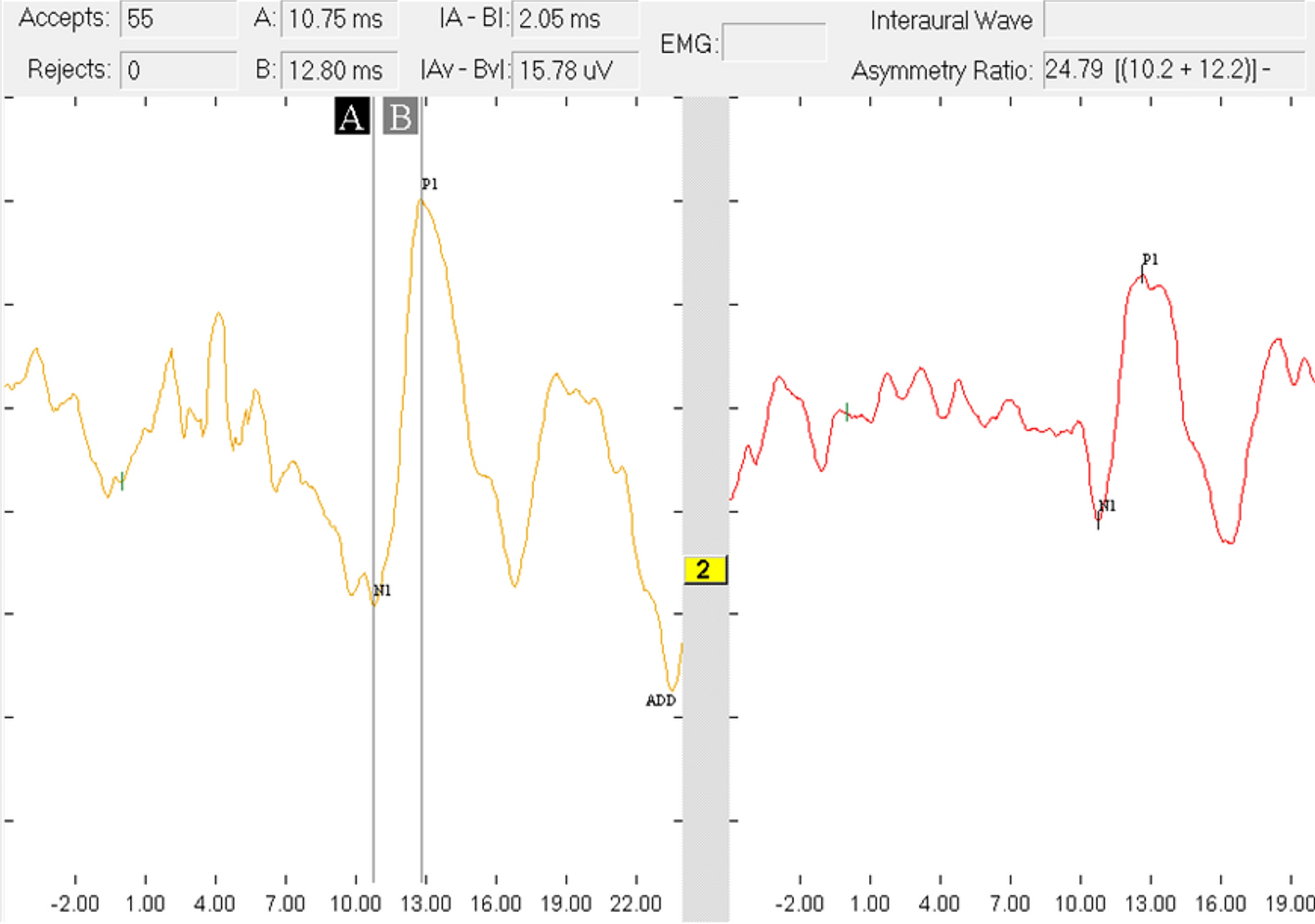
There are several studies comparing 500 Hz TB and 500 Hz Chirp stimuli in AC cVEMP and oVEMP. Murofushi et al. (2020) observed a shortening in p1 latency and a decrease in p1n1 amplitude with chirp stimulus. They found no significant difference between the two stimuli in terms of response rate [16]. Ocal et al.(2021) reported shorter p1 and n1 latencies with a larger p1n1 amplitude [17]. We obtained similar results with BC Chirp in accordance with the findings of Ocal et al. Aydın et al. (2021) also compared TB and Chirp stimuli in both oVEMP and cVEMP and obtained shorter p1 and n1 latencies, higher p1n1 amplitude, and higher response rate with Chirp stimulus [18]. However, as far as we know, there is no publication comparing BC 500 Hz TB and Chirp stimuli.
Çoban et al. (2021) compared 500 Hz TB and 500 Hz NB Chirp stimulus in BC oVEMP test and observed a shortening in n1 and p1 latencies and an increase in n1p1 amplitude with Chirp stimulus [12]. Similarly, we obtained shorter p1 and n1 latencies and higher p1n1 amplitude with Chirp stimulus. The results can be explained using numerous facts. One of the basis is that the tone burst stimulus has a substantially longer rise/fall time, which reduces its potency. Unlike tone bursts, chirp stimuli have no rise/fall time. The latency of reactions in BC oVEMP is made up of three components: bone conduction through the skull, transit time inside the utricle, and neural response. Çoban et al. stated that Chirp stimulus has a better stability than TB stimulus. They also suggested that the long latencies and low amplitudes obtained with TB stimuli may be due to frequency scattering [12]. The same may be possible in our study.
The main limitation of this study is that BC stimulation not only stimulated the saccule but also the utricle, thus obtaining a whole otolith organ response.
Compared to 500 Hz TB stimulus, 500 Hz Chirp stimulus results in higher response rate, larger p1n1 amplitude and shorter p1 and n1 latency. A larger wave amplitude may increase the recognizability of the waves, facilitating threshold determination. A higher response rate may provide more accurate assessment of otolith organs, reducing false negatives due to signal transmission in patients.



留言 (0)