This study aims to describe the audiological and psychometric profile of patients with chronic tinnitus and rare variants in the ANK2 gene. This study includes 12 patients reporting persistent severe tinnitus (THI > 56) since the onset of the disease; given that tinnitus may undergo variations over time, not all scores obtained during the duration of this study showed values > 56. However, our findings have demonstrated the persistence of high scores in the THI throughout the follow-up of most of these patients (83%).
Tinnitus is a common symptom in some diseases, but its closest relationship is undoubtedly established with hearing loss, including high-frequency sensorineural hearing loss, presbycusis, and Meniere’s disease (MD) [7]. In our series, 10 out of 12 patients were diagnosed with definite MD. Although more individuals with variants in ANK2 need to be studied, we cannot rule out an effect of ANK2 in hearing or vestibular loss in addition to tinnitus.
In addition to hearing impairment, other common psychological comorbidities such as depression, anxiety, insomnia, and cognitive impairment are present in 10–50% of tinnitus patients [23]. According to this, the standard assessment of these patients should include a complete audiological evaluation, psychoacoustic measures of tinnitus, and standardized questionnaires to determine the severity and its impact on health-related quality of life. Our study included the VAS scale as a reliable tool for measuring intensity, discomfort, and tinnitus-related distress [15]. In addition, the THI questionnaire was used to assess tinnitus severity and its functional impact on daily life [24]. THI and VAS scores show extreme annoyance values and a significant impact on the patient’s quality of life concerning tinnitus in more than half of the patients studied.
Depression and anxiety are commonly identified as contributing factors to the degree of distress in tinnitus sufferers [25]. Recently, De Ridder et al. proposed the concept of “tinnitus disorder” as distress associated with the conscious perception of noise, such as emotional distress, cognitive dysfunction, and autonomic excitation [2]. The literature has demonstrated the close relationship between depression and tinnitus [26, 27]. Bhatt et al. [28] reported a significantly higher prevalence of depression in patients who had suffered tinnitus in the last 12 months compared to those without tinnitus. They also demonstrate a higher prevalence of patients with both anxiety and tinnitus compared to the rates of patients with anxiety and no concomitant tinnitus, and they conclude that this association carries a strong relationship between tinnitus severity and the likelihood of anxiety and depression. Shargorodsky et al. [1] showed that about 50% of patients with anxiety disorders might suffer from tinnitus and that the prevalence of these disorders in tinnitus patients is higher compared to the general population.
To assess anxiety and depression, we have used the PHQ-9 scale, which is accepted as the best tool to identify the severity of symptoms in people with depressive disorder, and the HADS scale, which includes two subscales for anxiety and depression traits. Our results show that 58% of the patients presented symptoms of moderate to severe depression through the PHQ-9. However, only 42% of the patients presented relevant symptoms consistent with major depression in the HADS depression subscale, and 67% of patients showed anxiety symptoms based on the HADS anxiety subscale. As our sample includes patients with extreme phenotypes, these selection strategies are usually related to obtaining high scores in this type of psychometric test [7]. In addition, it is essential to note that the anxiety subscale of the HADS screens for anxious symptomatology with independence of its association with tinnitus. However, these questions can be easily related to feelings of tension, worry, or fear associated with tinnitus and not to a diagnosis of a generalized anxiety disorder.
Another relevant symptom observed in ANK2 tinnitus patients was reduced tolerance to environmental sounds, also known as hyperacusis, in which the sounds are uncomfortably loud or painful, ultimately impairing social, occupational, and recreational activities [29]. Over 90% of people with hyperacusis report concurrent tinnitus, suggesting a strong relationship [30], and this relationship increases with tinnitus severity [31]. In our case series, all patients had hyperacusis related to their tinnitus, and 75% showed a high annoyance based on the THI score.
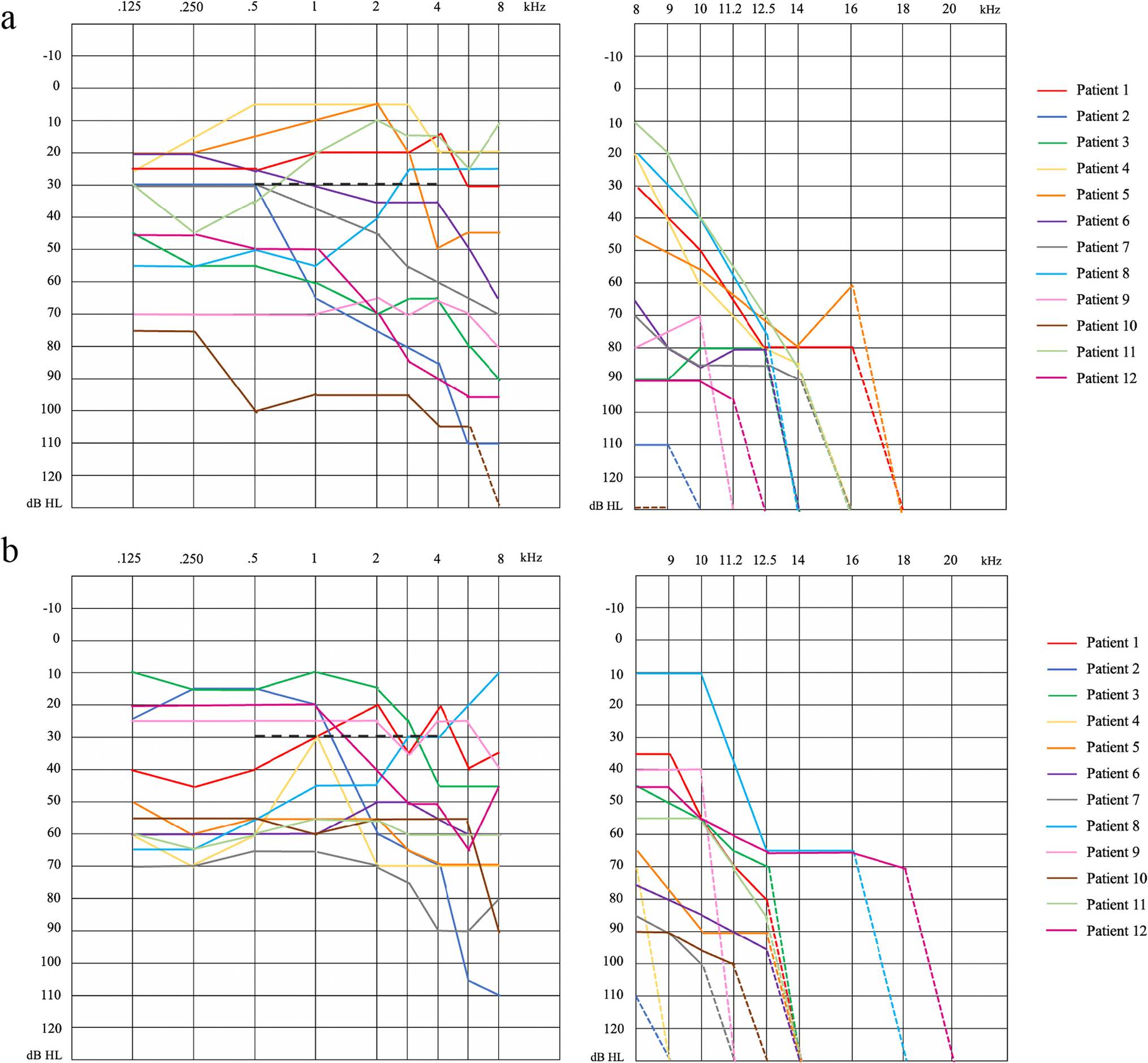
Cognitive impairment has been described in samples of tinnitus patients, and the severity of these symptoms has been correlated with the severity of tinnitus [32,33,34]. Wang et al. [35] demonstrated that the cognitive impairment occurring in patients with severe tinnitus was different from those occurring in patients with mild tinnitus, regardless of the degree of hearing loss, and suggested that the cognitive impairment may not secondary to the disease manifestations but a primary feature of the underlying disease. Melesci et al. [36] observed that in elderly patients with hearing loss, tinnitus appears to worsen cognitive dysfunction but concluded that it was still unclear whether cognitive impairment was a response to the manifestations of tinnitus or a feature of tinnitus in relation to age-related hearing loss. Our study used the MoCA test to detect mild cognitive dysfunctions. All of the patients from our series had bilateral hearing loss in different degrees, except for two patients with mild and moderate unilateral hearing loss. More than half of these patients had scores suggestive of mild cognitive impairment, with a lower mean age compared to the subgroup of patients without signs of cognitive impairment. However, we have not found statistically significant differences, probably due to insufficient sample size.
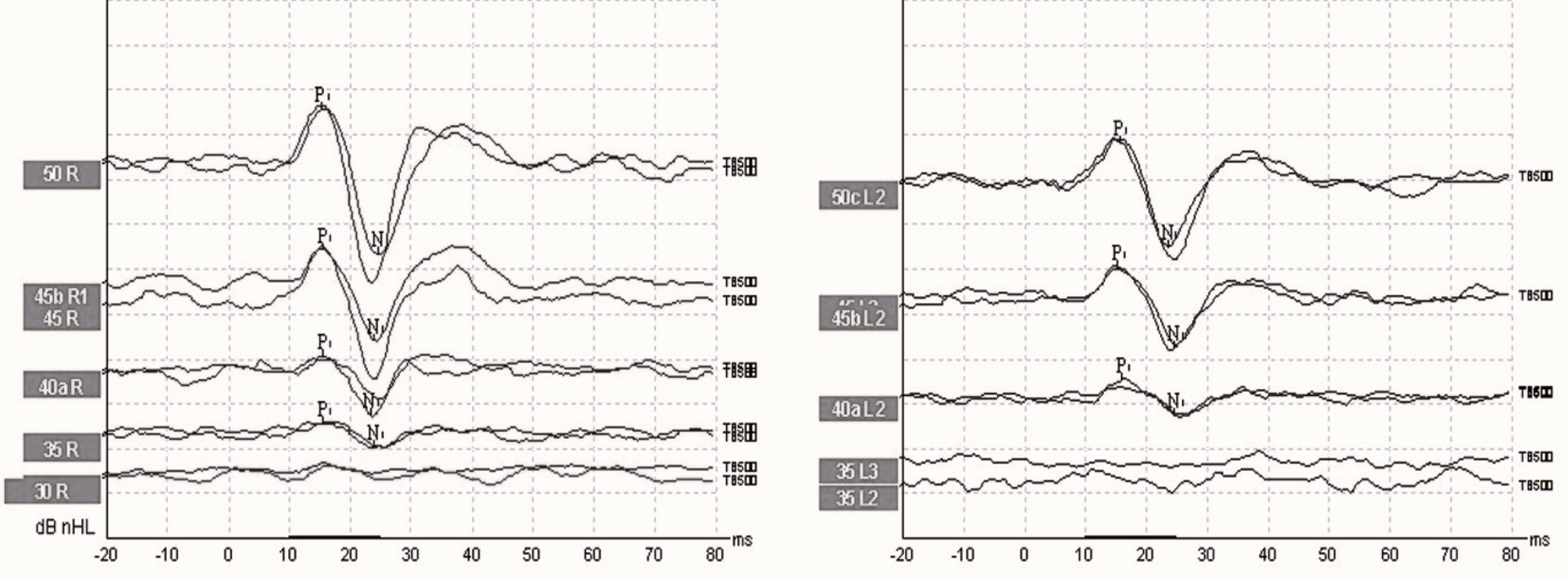
Average latency and amplitude data have been described for the different components of the ABRs [37]. However, depending on the hearing threshold, these values could vary in patients with hearing loss. It is now suggested that tinnitus arises as a dysfunction of central plasticity in response to decreased auditory sensory input after hearing damage. This leads to changes in the homeostatic control of gain in the auditory brainstem and auditory cortex and thalamocortical dysregulation [38]. Most of the patients in our series had bilateral hearing loss. In all cases, the ear affected by tinnitus also had different degrees of hearing loss. Edwall et al. [39] have described changes in the latencies and amplitudes of wave V in patients with chronic tinnitus as a result of the centrifugal effect of the auditory cortex [40] and subcortical brain structures beyond the brainstem. In our study, we observed a delay in the latencies of waves I, III, and V of the ears affected by severe tinnitus and a decrease in the amplitudes of waves I and V compared to the values obtained in the ears without tinnitus. Despite not showing statistical significance, these results align with the meta-analysis published by Milloy et al. [41], which described a generalized latency delay and amplitude decrease in the ABRs of tinnitus patients.
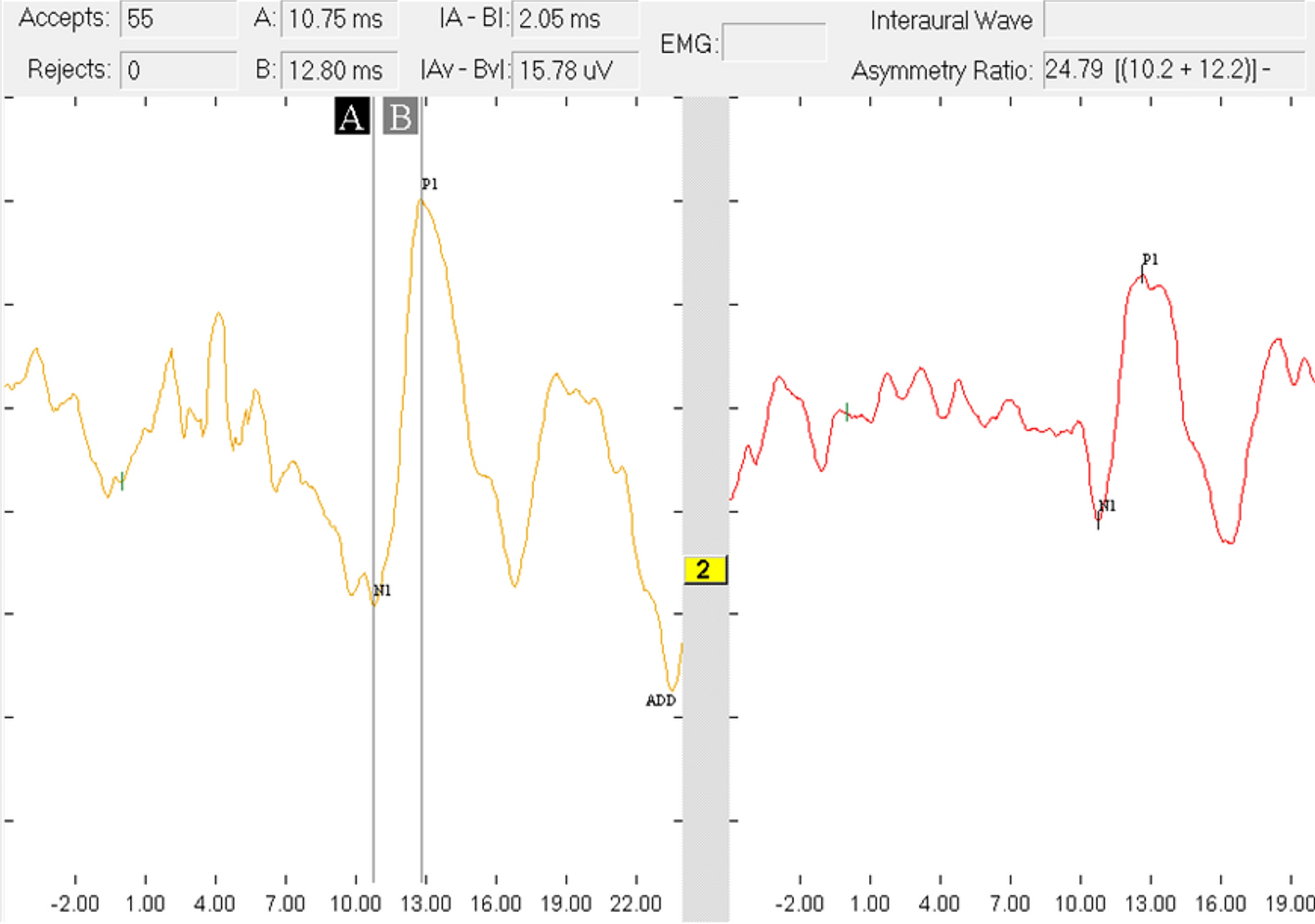
Although the role of cortical and subcortical auditory structures in the physiopathology of tinnitus needs to be better defined, only some studies have analyzed the role of AMLR latencies and amplitudes in tinnitus patients. Studying this type of mid-latency neural response can provide crucial information on the connection between the auditory pathways at the thalamocortical level and the mechanisms of corticolimbic dysfunction related to the degree of distress perceived by the patient with chronic severe tinnitus. Although the results are not statistically significant, our series shows delayed latencies in all AMLR components (Pa, Pb, and NaPb) of the ears with tinnitus. On the other hand, the amplitude of the main component of these auditory responses, Pa, is found in our series to be significantly increased in the tinnitus ears. It has been proposed that AMLRs may be a marker of tinnitus severity since both delayed latencies and increased amplitudes in diseased ears could reflect a malfunction of synchronized activity in subcortical and cortical regions [42].
Limitations
The authors are aware of the limitations of this phenotyping study, including the low sample size, but participants were only selected if they had rare variants in the ANK2 gene. This case series is focused on the analysis of patients with tinnitus extreme phenotype and rare variants in the ANK2 gene, and these results cannot be extended to the general population. Furthermore, a control group to compare our results with a group of patients with defined MD will be needed to confirm the phenotype's audiological, psychoacoustic, and psychometric features.



留言 (0)