One of the main pitfalls in allergy diagnostics is the influence of medication taken prior to testing. To prevent confounding effects on test outcomes, the intake of systemic antihistamines, for instance, is recommended to be discontinued for a minimum of seven days preceding in vitro or in vivo testing [11]. However, there are no recommendations nor empirical data concerning the management of monoclonal antibodies within this context. Nevertheless, this issue is on the rise as the utilization of Dupilumab and other biologics expands in the management of CRSwNP [12, 13]. Given the frequent co-occurrence of AR alongside CRSwNP of type 2 endotype [14] there is a discernible increase in the prevalence of conducting allergy diagnostics within the framework of Dupilumab treatment.
Via its subcutaneous route of administration Dupilumab achieves peak serum concentration within 3 to 7 days. Notably, it exhibits a relatively long half-life, approximately ranging from 17 to 20 days [15]. With a recommended administration rate of once every 14 days, a waiting period prior to allergy testing does not seem feasible only leaving the possibility of performing allergy diagnostics under ongoing biologic therapy. The present data aimed to assess potential limitations of allergy diagnostics if performed under Dupilumab treatment which is in our clinic the therapeutic choice for nearly 95% of the patient population with uncontrolled CRSwNP.
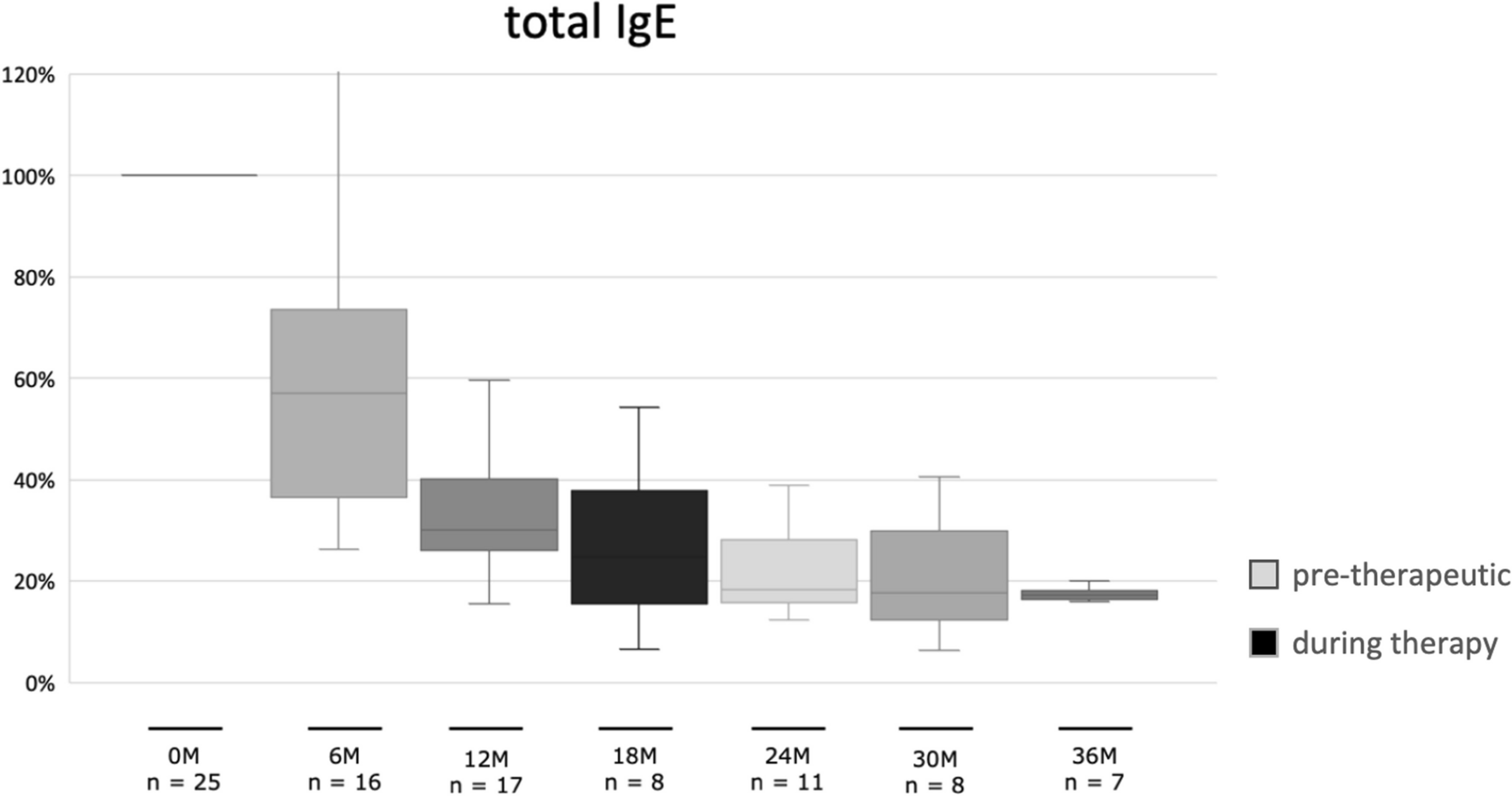
A comprehensive analysis of immunological parameters was available in a cohort of 25 patients, assessed over an average observation period of 28 months. Evaluation of tIgE levels revealed a substantial decline in IgE concentrations, approaching nearly 50% reduction six months following the commencement of biologic therapy. This is in line with published data where Dupilumab through its inhibiting of IL-4 and IL-13 has been shown to lead to a substantial reduction in tIgE typically occuring within the first few months of treatment [16]. Further, our data confirm that Dupilumab does not only reduce tIgE, but also sIgE against airborne allergens as already shown with respect to several food allergens by Spekhorst et al. [17]. Interestingly, evaluation of the quotient of sIgE and tIgE concerning various major inhalant allergens demonstrated no statistically significant reduction of the quotient of sIgE in tIgE in all analyzed allergens e.g. HDM, betulaceae, poaceae, and animal dander. The pivotal question is whether reducing tIgE concentrations might lead to a decrease in sIgE antibodies to the point where it becomes challenging to detect systemic sensitization using the ImmunoCAP test for allergy diagnostics. The concern is that this situation could result in overlooking important sensitizations with clinical significance.
Therefore, were further investigated the data of sIgE sensitizations. Considering recovery rates, as indicated by the presence of a CAP class ≥ 1 for IgE antibodies directed against the primary and substantial allergens encompassing poaceae, betulaceae, HDM, and animal dander a relatively high detection rate of 82% and 86% is evident for grass and birch pollen allergens respectively. In stark contrast, the CAP class system detected pre-existing sensitization to house dust mite (HSM) in only 75% of the cases and to animal dander in a mere 46% of cases. This implies that, conversely, a house dust mite sensitization might go unnoticed in 25% of cases, and a sensitization to animal dander could be overlooked in 54% of cases. It is imperative to recognize that a CAP class of 0 does not inherently signify the absence of sIgE antibodies. Indeed, when employing a detection threshold of > 0.1 kUA/l as the cut-off value, evidence of pre-existing sensitization to the major allergens in grasses and birch trees remains detectable in 100% of cases for each allergen under the influence of Dupilumab. Furthermore, in the context of house dust mite sensitization, this remains true in 83% of the cases, and sensitization to animal dander remains discernible in 73% of cases during the course of Dupilumab therapy. Overall, with regard to CAP class ≥ 1 a recognition rate of 73% was demonstrated, with stark contrast to a recognition rate of 89% when employing a detection threshold of > 0.1 kUA/l. This implies that when conducting allergy diagnostics via measurement of sIgE in the presence of Dupilumab, special emphasis should be placed on the absolute measurement of sIgE levels expressed in kUA/l. Relying solely on the categorization into CAP classes does not provide a robust basis for making conclusive assessments.
Upon establishing the viability of detecting sensitizations under treatment with biologics to a range of allergens through the quantification of sIgE directed against various allergenic components via the ImmunoCAP test, the question at hand pertains to the comparability and effectiveness of this method when compared to the conventional practices of skin prick testing and the utilization of standard Allergy Screening Panels, which are typically employed in initial allergy assessments.
Preceding the onset of biologic therapy, a total of 110 sensitizations to 15 aeroallergens were recorded employing the Allergy Screening Panel. These sensitizations were expressed semi-quantitatively in terms of CAP classes equal to or greater than 1. Following an average treatment duration of 28 months, it was observed that 83 of these sensitizations (75%) remained detectable, while more than a fourth of preexisting sensitizations were no longer recognizable. It is imperative to note that this diagnostic approach solely provides an assessment of sensitization categorized in CAP classes without offering quantification in terms of sIgE levels. Notably, among the 27 sensitizations that were not recognized, 16 initially fell into a CAP class of 1 prior to biologic treatment, implying a potential limitation of the screening tool, particularly in cases of lower sensitization levels. In contrast, the data derived from the Skin Prick-Test (SPT) revealed that 94 out of the initial 96 sensitizations (98%) endured throughout the patients' course of biologic therapy. Only two sensitizations, deemed of minimal clinical significance and related to plantain and cat allergens, were not detectable in two distinct patients. It is crucial to underscore that our investigation specifically assessed sensitizations rather than allergies. Therefore, one might hypothesize, that the recognition rate of clinically manifest allergies might be even higher, as most undetected sensitizations had a pre-therapeutic low sensitization level making them more likely to lack clinical relevance [6].
Our findings suggest that SPT may offer a more consistent and comprehensive assessment of sensitizations under biologic treatment, as confirmed by its superior recognition rate of sensitizations in comparison to the Allergy Screening Panel. While the applicability of these observations to other commercially available test kits remains speculative, it is conspicuous that SPT stands out as a precise diagnostic tool in the context of detecting sensitizations to allergens during Dupilumab treatment.
Another limitation of this study is the uneven temporal follow-up of the patient sample. While a minimum follow-up of 20 months for the ImmunoCAP test seems sufficient, the occasionally shorter follow-up timepoints for SPT and Allergy Screening may introduce a bias and skew the results.
While Dupilumab has demonstrated its efficacy as an adjunct treatment for patients with uncontrolled persistent asthma and comorbid AR [18], it is essential to emphasize that the primary objective of this study was not to assess the clinical benefits or therapeutic effects of Dupilumab in the context of AR. While this topic certainly warrants further investigation, the primary focus of our study was to evaluate whether ongoing treatment with Dupilumab has any impact on allergy diagnostics conducted in routine clinical practice. Therefore, we can assert that, while acknowledging the inherent limitations and challenges, allergy diagnostics during antibody therapy with Dupilumab certainly remains viable and feasible.



留言 (0)