
記住我


Since its initial proposal, TPAB has been extensively utilized in abdominal surgery, and TAPB has also demonstrated analgesic effects in bariatric surgery [9]. In this study, TAPB is chosen as the control group, rather than a blank control group, based on its analgesic effect advantage, which can maximize the benefits for patients. Furthermore, choosing TAPB as the comparator is more appropriate because the study aims to explore management strategies that are more effective in relieving the pain associated with bariatric surgery, thus requiring a comparison with proven effective pain management strategies. However, due to its limited mechanism of action, TAPB can only alleviate incisional pain rather than visceral pain, which is precisely the advantage of subcostal anterior QLB. There is currently a dearth of prospective clinical studies comparing the analgesic efficacy of TAPB and anterior subcostal QLB in obese patients.
Intervention description QLB groupIn the surgical setting, researchers will adhere to standardized protocols for monitoring participants’ vital signs. Participants will be instructed to assume a supine position. Subsequently, the researchers will meticulously sterilize and drape the surgical site before positioning the low-frequency probe at an angle of 6–8 cm outside the L1–2 spinous processes, on the lateral aspect where the erector spinae muscle and iliocostalis muscle intersect. It will be observed that the quadratus lumborum muscle is below the 12th rib margin, where there are only latissimus dorsi muscle and serratus posterior inferior muscle behind the quadratus lumborum muscle, and there is the anterior layer of the thoracolumbar fascia, diaphragm, perirenal fat, and kidney in front of the quadratus lumborum muscle. Move the probe to the inside, and the latissimus dorsi muscle gradually thins until it disappears. At this time, the erector spinae muscle is located behind the quadratus lumborum muscle, and the psoas major muscle is located in front of it. The researchers will inject 3 ml of normal saline between the quadratus lumborum and the anterior layer of thoracolumbar fascia through the pump tube and puncture needle to confirm that the liquid diffuses in the target space. Then the drug solution of 0.25% ropivacaine will be given 30 ml. Afterwards, the researchers will replicate the procedure on the opposite side of the subject and then instruct them to assume a supine position. The researchers will use a bottle with ice to test the coverage of the skin layer with a sensory block. General anesthesia will be performed after the test (Fig. 2).
Fig. 2
The position of the patient preparing for subcostal anterior QLB and the placement of the ultrasound probe. Ultrasound images of anatomy, needle targets, and injection points. QLM, quadratus lumborum muscle; kidney and pre-renal fat; 12th rib; POI, point of injection with needling path
If the researchers have difficulty or failure with the puncture, the trial will be terminated in accordance with standard procedures, and the participant will receive general anesthesia. Subsequently, they will undergo follow-up until discharge to assess any potential adverse events resulting from a failed nerve block.
TAPB groupIn the surgical setting, researchers will adhere to standardized protocols for monitoring participants’ vital signs. Participants will be instructed to assume a lateral recumbent position. The researchers will place the ultrasound probe vertically above the iliac crest and move the probe upwards once they see the iliac crest. From the outside to the inside, the researchers will see the fat layer, external oblique muscle, internal oblique muscle, and transverse muscle. The researchers will employ a puncture needle to penetrate from the front/inside direction, passing through the fat layer, external oblique muscle, and internal oblique muscle. The needle tip will be located at the superficial part of the transverse abdominal fascia. Three milliliters of normal saline will be given through the pump tube and puncture needle to confirm the liquid diffusion in the target space. Then the drug solution of 0.25% ropivacaine will be given 30 ml. Afterwards, the researchers will replicate the procedure on the opposite side of the subject. The researchers will use a bottle with ice to test the coverage of the skin layer with a sensory block. General anesthesia will be performed after the test (Fig. 3).
Fig. 3
The position of the patient preparing for TAPB and the placement of the ultrasound probe. Ultrasound images of anatomy, needle targets, and injection points. EOM, external oblique muscle; IOM, internal oblique muscle; TM, transverse muscle; TAP, transversus abdominis plane; POI, point of injection with needling path
If the researchers have difficulty or failure with the puncture, the trial will be terminated in accordance with standard procedures, and the participant will receive general anesthesia. Subsequently, they will undergo follow-up until discharge to assess any potential adverse events resulting from a failed nerve block.
Criteria for discontinuing or modifying allocated interventionsThe criteria for withdrawal from the trial are as follows: (1) If participants request to withdraw from the trial prior to successful implementation of the nerve block, researchers will provide standard treatment and cease data collection. Once the nerve block is successfully implemented, participants will no longer be able to withdraw from the trial. (2) Due to unforeseen circumstances (such as failure in performing nerve block), the researchers reserve the right to terminate the study.
Strategies to improve adherence to interventionsComprehensive informed consent process: During the recruitment stage, it is essential to ensure that participants are provided with well-defined, comprehensive, and easily comprehensible informed consent documents. These documents should encompass detailed information on the study objectives, procedures, potential risks, and benefits. It is imperative to confirm that participants have a full understanding of the study and participate voluntarily. Meanwhile, the researchers will inform the patients that once the nerve block is successfully performed, they will not be able to decline participation in the trial.
Collaborative efforts by medical teams: Effective collaboration among members of the medical team should be ensured to address potential issues affecting adherence. A cohesive medical team can proficiently tackle challenges related to participant adherence.
Privacy and data protection measures: Participants must be assured of robust data protection measures and efforts made towards ensuring anonymity where feasible. This approach serves to allay concerns and bolster trust in the research process among participants.
Relevant concomitant care permitted or prohibited during the trial Induction and maintenance of anesthesiaIrrespective of group allocation, the anesthesia induction protocol consisted of propofol 2 mg/kg, sufentanil 0.4 μg/kg, rocuronium 0.6 mg/kg, and dexamethasone 5 mg under general anesthesia. The doses of propofol and rocuronium will be calculated based on the patient’s total body weight, while the dose of sufentanil will be determined by the lean body weight (LBW): male LBW (kg) = 9270 × ideal body weight (kg)/(6680 + (216 × BMI (kg/m2)), female LBW (kg) = 9270 × ideal body weight (kg)/(8480 + (244 × BMI (kg/m2)). After 3 min, intubate the trachea and perform mechanical ventilation. Adjust the parameters of the ventilator. The tidal volume (VT) is 6–8 ml/kg. The tidal volume is calculated according to the ideal weight. The ideal weight (kg) = height (cm) − 105 (female 100). The respiratory rate is adjusted based on the end-tidal carbon dioxide level and maintained within the range of 35–45 mmHg. The pneumoperitoneum pressure is set to 12 mmHg. Administer sevoflurane and remifentanil for maintenance of general anesthesia, while ensuring the bispectral index remains within the range of 40 to 60. Blood pressure is regulated to stay within 20% of baseline levels. Muscle relaxation is achieved through intermittent intravenous injection of rocuronium. Ten milligrams of azasetron and 50 mg of flurbiprofen are administered via intravenous injection 20 min before the end of the surgery. After the surgical procedure, both groups received patient-controlled intravenous analgesia (PCIA). The PCIA regimen consisted of sufentanil 100ug diluted in 100 ml of normal saline to achieve a concentration of 1 μg/ml. There was no background dose and a single bolus dose of 5 ml with a lock-in time of 15 min and a limiting dose of 20 ml/h. The PCIA medication would be replenished as needed for up to 48 h post-operation.
The patient was transferred to the post-anesthesia care unit (PACU) following the surgical procedure, where continuous monitoring of vital signs will be conducted throughout the recovery period. In PACU, the severity of pain at rest and during activity will be assessed by the visual analog scale (VAS) (0 = no pain, 10 = the most severe pain imaginable). If PCIA is fully utilized but significant surgery-related pain persists, additional injections of sufentanil at a dose of 5 μg each time may be administered until the VAS score is ≤ 3.
PONV during PACU will be treated by intravenous injection of 1 mg of droperidol. The patient will only be transferred to a ward once they no longer experience postoperative nausea or vomiting.
The postoperative treatment protocol for patients in the ward is as follows: during the initial 48-h period following surgery, patients will be administered PCIA therapy in conjunction with a 50-mg intravenous infusion of flurbiprofen every 12 h. If the patient’s VAS remains ≥ 4 within this timeframe, an intravenous injection of 100 mg tramadol may be given, with a maximum daily dosage not to exceed 400 mg.
Provisions for post-trial careIn the event of a participant experiencing a complication related to the intervention, a multidisciplinary team consisting of surgical, anesthesia, and nursing professionals will provide standard postoperative management. Additionally, our team will closely monitor participants throughout their hospitalization to ensure freedom from potential complications and to deliver timely treatment as necessary. Our aim is to ensure that all participants receive the highest quality of treatment and care during the trial.
Outcomes Primary outcomeAs the primary outcome, we will evaluate the consumption of opioids 24 h after surgery.
Secondary outcomesThe secondary outcomes included the following: (1) VAS of pain during rest/activity at 2, 4, 6, 12, 24, and 48 h after operation (the score during activity will be evaluated by cough); add the type and dose of analgesics; (2) incidence and severity of nausea and vomiting at 2, 4, 6, 12, 24, and 48 h after operation(VAS); add the type and dose of antiemetic drugs; (3) PACU time; (4) time of first flatus postoperatively; (5) time of first ambulation postoperatively; (6) Time of first liquid diet postoperatively; and (7) postoperative admission days.
Participant timelineThe schedule for enrollment, intervention, and evaluation is depicted in Figs. 1 and 4.
Fig. 4
SPIRIT figure. Standard Protocol Items: Recommedations for Interventional Trials (SPIRIT). h, hours; QLB, quadratus lumborum block; TAPB, transversus abdominis plane block; VAS, visual analog scale
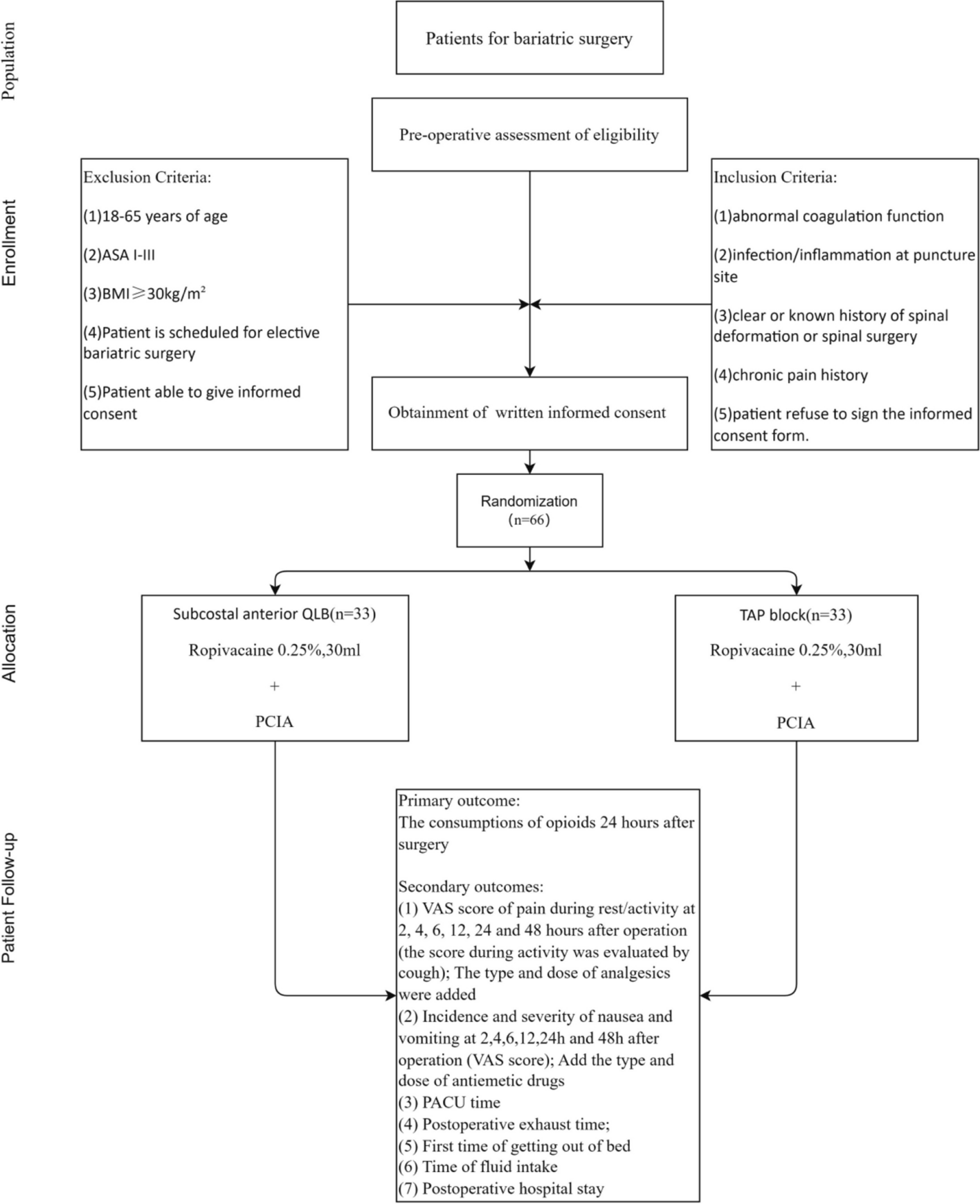
Sample size calculationIn the preliminary trial, we administered TAPB for postoperative analgesia to 10 patients who underwent bariatric surgery. The average consumption of sufentanil during the first 24 h after surgery was 56.5 (SD = 15.4) μg. We used the software of PASS 2021 to calculate the sample size. We hypothesized that the use of subcostal anterior QLB for postoperative analgesia in patients undergoing bariatric surgery would result in a 20% reduction in sufentanil consumption compared to the TAPB group, with a significance level of α = 0.05. With an inspection efficiency of 1 − β = 0.80 and a 1:1 grouping, we calculated that 30 patients are required for each group. Requiring a 10% allowance for lost cases, each group will need 33 patients, resulting in a total of 66 patients needed for the study.
RecruitmentParticipants will be recruited via social media platforms (e.g., WeChat), promotional materials, and online news outlets. Furthermore, a variety of recruitment strategies will be employed, including in-person invitations during clinic visits and referrals from various medical disciplines. Following participant selection, research personnel will assume responsibility for identifying and enrolling eligible individuals who meet the inclusion criteria.
留言 (0)