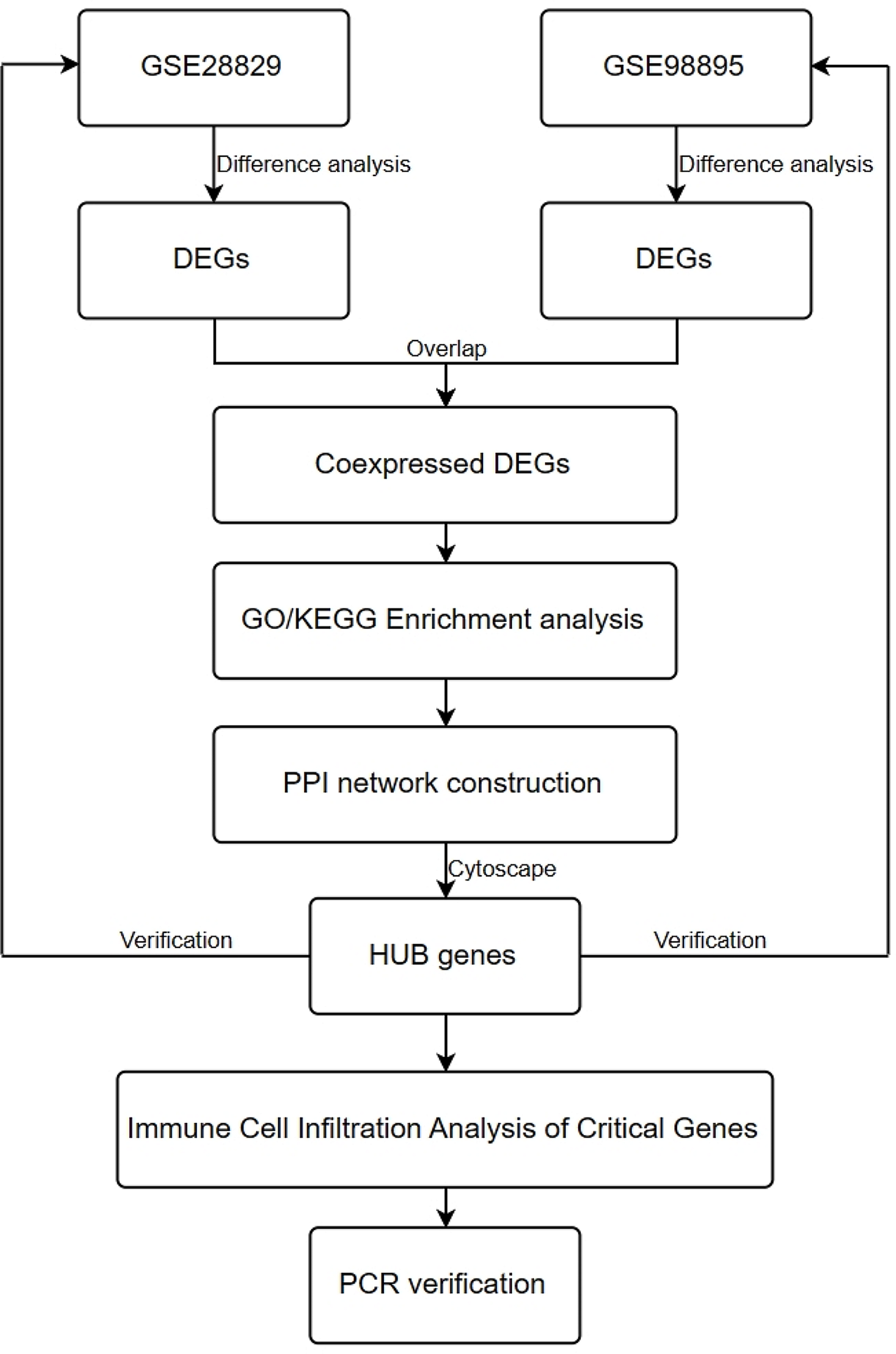
There is a close relationship between atherosclerosis and metabolic syndrome. MS plays an important role in the occurrence and development of AS. MS is a multiple risk factor for atherosclerotic cardiovascular disease, but the specific relationship between MS and AS is not completely clear.In our study, we used GEO database to obtain common differential genes between AS and MS through difference analysis, and used GO/KEGG functional enrichment analysis to explore their possible related biological processes. Then we established a PPI interaction network and identified 10 hub genes using Cytoscape software. Finally, we performed PCR in GEO database and plasma of metabolic syndrome patients with atherosclerosis to further verify the screened hub gene. Finally, we screened 10 hub genes, and there were significant differences among patients with AS complicated with MS.
Atherosclerosis refers to the accumulation of fat and / or fibrous substances in the innermost layer of the artery, namely intima. Over time, atherosclerotic plaques become more fibrous and accumulate calcium minerals. Late atherosclerotic plaques can invade the arterial lumen, hinder blood flow, and lead to tissue ischemia. Atherosclerosis, which does not produce flow-limiting blockage, destroys and causes thrombosis, which blocks the lumen, providing a second pathway to ischemia, usually more acute. Atherosclerotic cardiovascular disease (CVDs) is still the leading cause of vascular disease worldwide. When it affects the circulation of the heart itself, it can cause acute coronary syndrome or chronic diseases, including myocardial infarction, such as stable angina pectoris (chest pain or discomfort caused by insufficient myocardial perfusion). Atherosclerosis causes many ischemic strokes and transient ischemic attacks. It can lead to the formation of aneurysms, including those on the abdominal aorta. When it affects the peripheral artery, it can cause intermittent claudication, ulcers and gangrene, endangering the viability of the limbs [15].
MS is a multiple risk factor associated with metabolic abnormalities [16]. MS is characterized by a series of interrelated risk factors for atherosclerosis, including insulin resistance, hypertension, abdominal obesity, impaired glucose metabolism and dyslipidemia, which share the risk of ASCVD.Having three or more of these ingredients will make it possible for a person to have MS [17]. Detailed understanding of the components of MS is essential for the development of effective prevention strategies and appropriate intervention tools, which can curb its increasing prevalence and limit its complications.Hyperglycemia is considered to be a component of MS. It is described as a steady state with higher-than-normal plasma glucose levels after overnight fasting.The underlying pathophysiological mechanism is the interaction between pancreatic β-cell dysfunction and peripheral and hepatic IR, which leads to abnormal hepatic glucose production [18]. Due to the use of insulin or hypoglycemic drugs, diabetic patients rarely die of hyperglycemia; on the contrary, 75% of diabetic patients die directly from cardiovascular disease [19]. The risk of cardiovascular disease in patients with diabetes is 2–4 times higher than that in the general population [20]. Hypertension is another important component of MS, which exists in up to 1/3 of MS patients.There is evidence that even if there is no T2DM, MS can increase the risk of cardiovascular morbidity and mortality in patients with hypertension [21]. Blood pressure level is closely related to visceral obesity and insulin resistance, which is the main pathophysiological feature of MS. The higher level of systolic blood pressure may reflect the progressive hardening of arterial wall, the change of vascular structure and the development of atherosclerosis [22]. Obesity is a multifactorial chronic disease characterized by fat deposition in new adipocytes and enlargement of existing cells [23]. Obesity is a chronic inflammatory state that produces a variety of cytokines and inflammatory markers that increase the risk of cardiac metabolism and metabolism-related diseases [24, 25]. Obesity can be quantified by body mass index (BMI), which is determined by weight (kg) divided by height squared (m2) (kg/m2). The BMI index is determined by weight (kg) divided by height squared (m2). A better way to define obesity is by the percentage of total body fat [26]. Body fat percentage measurements are rarely used because of inconvenience and cost, so the best way to estimate obesity is to calculate the waist circumference (WC). This is because excessive abdominal fat is closely related to metabolic risk factors.Waist circumference ratio (WHR) is an alternative indicator of central obesity. Compared with BMI [27] and WC [28], WHR is a superior indicator of CVD risk. Studies have shown that each additional unit of BMI increases the risk of cardiovascular disease by 8 per cent [29]. In addition, for every 0.01 unit increase in waist width ratio for both men and women, the risk of cardiovascular events increased by 5% [28]. Therefore, these simple indicators of abdominal obesity should be included in the risk assessment of cardiovascular disease. Weight control through lifestyle changes is considered to be an effective strategy to achieve and maintain a healthy weight.Lipid abnormality is a sign of MS, which is characterized by an increase in plasma triglyceride concentration, a decrease in high density lipoprotein cholesterol (HDL-C) and an increase in low density lipoprotein cholesterol (LDL-C).Dyslipidemia is generally considered to be an independent risk factor for atherosclerosis [30]. Low plasma HDL-C level and hypertriglyceridemia are independently and significantly correlated with myocardial infarction in patients with MS [31]. Therefore, in our study, we found 10 meaningful hub genes between the common differentially expressed genes of AS and MS, and verified by PCR by collecting relevant clinical blood samples. the results showed that there were significant differences in hub genes between patients and non-patients. We focused on the three key genes we verified.
CX3CR1 is the receptor of CX3CL1, which is a G protein coupled receptor (GPCR). It has seven transmembrane (TM7) transmembrane regions. Under the condition of flow in vitro, CX3CR1 receptor can mediate the tight adhesion of cells to fixed fractalkine. CX3CR1 exists in many early leukocyte cells, and CX3CR1-CX3CL1 signal transduction plays different functions in different tissue regions, such as immune response, inflammation, cell adhesion and chemotaxis [32]. CX3CR1-CX3CL1 signal transduction mediates cell migration function (through similarity). Responsible for recruiting natural killer (NK) cells into inflamed tissue (through similarity).Promote cell survival (through similarity) by mediating macrophages and monocytes to recruit inflamed atherosclerotic plaques as regulators of the inflammatory process that leads to atherosclerosis. CX3CL1 and CX3CR1 play a role in many inflammatory diseases. It has been suggested that CX3CR1 participates in the pathogenesis of these diseases by promoting the migration of monocytes or lymphocytes expressing CX3CR1. In contrast, the role of CX3CR1 and atherosclerosis has been clearly confirmed [33, 34].
Interleukin-32 (IL32) is described as a pro-inflammatory cytokine, which is involved in the pathogenesis of many inflammatory diseases. It is known to play a role in rheumatoid arthritis because it can induce TNF α, a major cytokine in Rheumatoid Arthritis. In addition, IL-32 helps to induce other pro-inflammatory mediators, such as procoagulant, pro-inflammatory and cytokine effects of IL-1 β when siRNA reduces IL-32 levels, such as IL-1 β-induced ICAM-1 production, which also significantly reduces the up-regulation of ICAM-1 in human umbilical cord endothelial cells (HUVECs) induced by IL-1 β, so it is considered that IL32 plays an important role in the process of atherosclerosis [35, 36]. At the same time, IL-32 is also highly expressed in T cells and is known to play an important role in the late stage of atherosclerosis, characterized by plaque instability and rupture. In view of these facts, IL-32 is an important factor promoting the development of CVD in individuals with chronic inflammatory diseases.
TLR5 is the extracellular receptor of bacterial flagellin and is widely expressed in almost all tissue types.In addition to one or more exogenous stimuli, most tlr also respond to specific endogenous ligands [37]. Although most of the endogenous ligands of TLRs9 have been described, there is a lack of equivalent ligands for TLR5. Since many exogenous TLR ligands are expressed in atherosclerotic lesions, flagellin may also play a role in the development of atherosclerosis.Related studies show that TLR5 deficiency can reduce the formation of atherosclerosis in LDLr-/-mice [38]. In addition, the plaques of these mice contained fewer macrophages and smaller necrotic cores than mice that received WT bone marrow. These results are also expressed, that is, the role of TLR5 in atherosclerotic plaque formation and inflammatory cell accumulation [39, 40].
Atherosclerosis is increasingly regarded as an inflammatory disease because the inflammatory process plays an important role in all stages of plaque development. It is also considered as a possible mechanism for the adverse consequences of MS [41]. In fact, the level of inflammation in patients with MS may help identify patients who are at high risk of adverse consequences. Inflammation can increase OS by oxidative modification of LDL [42]. The immune response to these modified lipoproteins drives the pathogenicity of plaques by releasing pro-inflammatory mediators, leading to chronic inflammation. Oxidized LDL atherosclerotic products induce the formation of foam cells and fat stripes in the vascular wall, which is a sign of the beginning of atherosclerosis [43]. Therefore, in our study, we analyzed the immune infiltration of atherosclerosis and metabolic syndrome at the same time, and analyzed the correlation of immune infiltration of the screened hub gene.
However, our study still has some limitations, first of all, the data are derived from the GEO public database, rather than RNA-seq through patient specimens, there are some information differences. Secondly, this study is a single-center study, in the clinical verification stage of the sample, the sample size is limited, our results only select the more prominent three genes in the clinical samples for verification.In addition, further animal and cellular studies are needed to confirm the function and mechanism of these genes.

留言 (0)