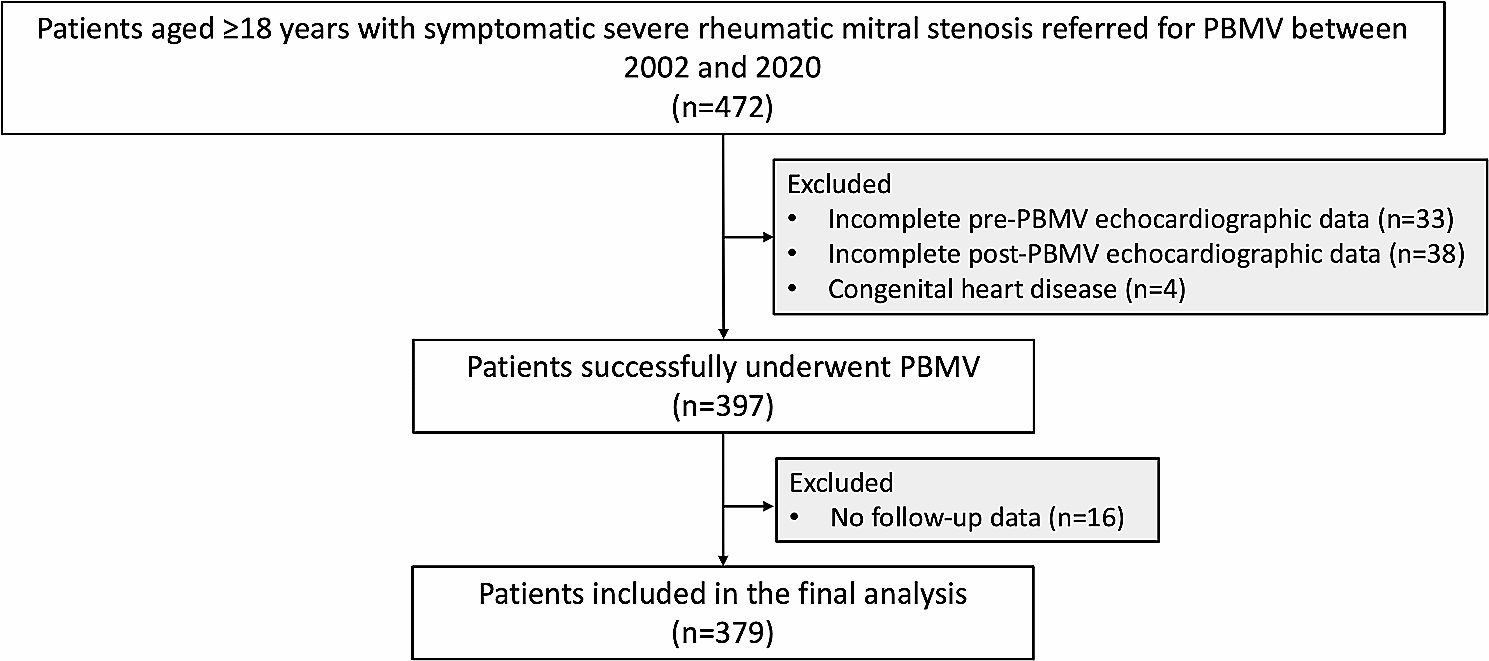
The main findings of the study were that during the median follow-up time of 5.9 years, 19.5% of patients with rheumatic MS undergoing PBMV experienced adverse cardiac outcomes, with an annualized event rate of 2.7%. Age, significant TR, immediate post-PBMV mitral valve area, and immediate post-PBMV MR were identified as independent predictors of adverse outcomes, with significant TR emerging as the strongest predictor.
Rheumatic heart disease remains a significant health concern in many parts of the world, particularly in low- and middle-income countries, where it is one of the leading causes of cardiovascular morbidity and mortality [14]. Ou et al. reported global trends in rheumatic heart disease, noting increasing trends in the age-standardized rates of incidence and prevalence worldwide. The respective estimated annual percentage changes were 0.58 and 0.57, with increasing trends commonly observed in low- and middle-socioeconomic countries [15].
PBMV should be considered as an initial treatment for selected patients who exhibit mild to moderate calcification or impaired subvalvular apparatus, but otherwise possess favorable clinical characteristics [16]. A recent meta-analysis showed lower procedural morbidity associated with PBMV compared with mitral valve replacement, thus supporting the recommendation of PBMV in young patients with suitable anatomy [17]. Several studies report long-term outcomes of patients with MS following PBMV, demonstrating an incidence of adverse outcomes ranging from 16 to 19% [5,6,7,8,9]. In our study, the incidence of adverse outcomes was comparable to prior studies, with a rate of 19.5%. Patients with adverse outcomes had a worse functional class and a greater left atrial dimension, which were also similar to previous studies [8, 9]. However, in our study, NYHA functional class was only a predictive factor in the univariable analysis. It should be noted that NYHA functional class, although a strong predictive factor for adverse outcomes, is a subjective variable. The clinical data from patients complaining of a defined NYHA functional class were assessed by physicians, which may result in differences in interpretation among patients.
Significant TR was the strongest predictor of adverse outcomes in our study, which was reported in prior studies. TR is most often the consequence of left-sided cardiac diseases that induce right-sided chamber dilatation, and hemodynamically significant TR can cause significant morbidity and mortality [18, 19]. Although rheumatic TR can occur, secondary TR due to pulmonary hypertension is far more common in patients with rheumatic heart disease. Significant TR can develop over time even after successful PBMV [20]. Sagie et al. studied the association between the presence of TR and immediate and late adverse outcomes in patients undergoing PBMV. They found that the prevalence of significant TR was 31%, and patients undergoing PBMV with significant TR exhibited advanced mitral valve and pulmonary vascular disease, suboptimal immediate results, and poor late outcomes [21]. Another study by Caldas et al. also showed that the prevalence of significant TR was 12.8% in patients with rheumatic MS undergoing PBMV and was independently associated with adverse outcomes [22]. Our study revealed a similar prevalence of significant TR to that reported by Sagie et al., but higher than that reported by Caldas et al. This difference could be attributed to variations in the definition of severity and the assessment methods used in the studies. Nevertheless, significant TR consistently emerges as a strong predictor of adverse outcomes in all studies, including ours.
Immediate post-PBMV mitral valve area has been associated with long-term outcomes in patients with rheumatic MS undergoing PBMV in prior studies [23, 24]. Our results also showed consistent findings. Significant MR following PMMV is a frequent event, mainly related to commissural splitting, with favorable clinical outcomes [25]. However, patients with damaged central leaflet scallop or subvalvular apparatus had the worst outcomes compared to patients with mild or commissural MR [26]. In our study, although we were unable to classify the severity or mechanism of immediate MR following PBMV, immediate post-PBMV MR still emerged as an independent predictor of adverse outcomes.
The clinical implication of our study is that PBMV in patients with severe MS demonstrated good long-term outcomes with a relatively low rate of adverse outcomes. Most adverse outcomes were mitral valve surgeries, with very low rates of mortality or heart failure. Additionally, our study highlighted significant known predictors of adverse outcomes, such as age, immediate post-PBMV mitral valve area, and immediate post-PBMV MR, as well as an emerging predictor, significant TR, which should be integrated into the care of this patient population.
Limitations
Our study had several limitations. Firstly, the study methodology was retrospective, and therefore, some confounding factors could not be totally eliminated. However, multivariable analysis was performed to the best of our ability. Secondly, the PBMV procedures were performed by experienced operators in a tertiary center, which may limit generalization. However, the rate of adverse outcomes in our study was comparable to prior studies. Thirdly, we were unable to conduct follow-up echocardiography after discharge, which could be associated with adverse long-term outcomes. Fourthly, we defined the severity of other valvular functions rather than MS using multiple methods, including qualitative and quantitative methods, and were unable to quantify the severity of other valvular functions (e.g., TR) in every patient, which may not be consistent.

留言 (0)