
記住我


At the time of the data cutoff, 5234 persons of childbearing potential (defined as female individuals aged 15–55 years) had received at least one dose of upadacitinib in a clinical study. A total of 97 maternal exposure pregnancies among 96 patients (one patient experienced two distinct pregnancies) with in utero exposure to upadacitinib were identified in the upadacitinib clinical trials across indications; of these 97 pregnancies, 17 were ongoing or lost to follow-up at the time of the data cutoff, leaving 80 pregnancies with known outcomes. Table 1 summarizes demographic and clinical characteristics at the start of the reported pregnancy (n = 80), stratified by disease indication. A table summarizing this information for all pregnancies, including those lost to follow-up or ongoing, is available in Table S3 of the ESM.
Table 1 Demographic and clinical characteristics at the start of pregnancies with known outcomes (n = 80) observed in clinical trialsThe age range of patients who became pregnant was 27–33 years, with a mean (standard deviation) age of 31.1 ± 6.2 years. At the time of pregnancy, more than half (63.8%) of patients had received their disease diagnosis ≥ 5 years prior. In total, 26.3% (n = 21/80) of patients were receiving concomitant methotrexate at the start of pregnancy, with a mean (standard deviation) dose of 16.4 ± 4.5 mg/week; all of these patients were enrolled in rheumatoid arthritis or psoriatic arthritis studies. About a quarter (n = 23, 28.8%) of patients were receiving concomitant oral corticosteroids (rheumatoid arthritis: n = 22; ulcerative colitis: n = 1), with a mean prednisone equivalent daily dose of 6.0 ± 3.7 mg.
Disease activity status varied by disease indication. More than half of patients with rheumatoid arthritis and psoriatic arthritis were in remission or had minimal disease activity at the start of pregnancy. Nearly all patients with non-radiographic axial spondyloarthritis (100%), atopic dermatitis (95.7%), and Crohn’s disease (100%) had achieved an inactive disease state or a state of disease control at the start of pregnancy. Only 40% of patients with ulcerative colitis were in clinical remission based on the Adapted Mayo Score.
3.1.2 Pregnancy Reports and OutcomesOf the 80 pregnancies with known outcomes, prospective (n = 69) and retrospective (n = 11) cases were combined because of limited numbers, with the majority being prospective, based on the nature of close monitoring for pregnancies during the clinical trials. The distribution of pregnancies across diseases was as follows: 34 with rheumatoid arthritis, 6 with psoriatic arthritis, 1 with non-radiographic axial spondyloarthritis, 23 with atopic dermatitis, 10 with ulcerative colitis, and 6 with Crohn’s disease. One patient with rheumatoid arthritis had two pregnancies while on upadacitinib treatment. The first pregnancy ended in spontaneous abortion and approximately a year later, the patient became pregnant after reentering the study and had a live birth without congenital anomaly.
Given the frequent pregnancy testing mandated during clinical trials, a pregnancy was generally detected during the first trimester of pregnancy (< 13 weeks). In this analysis, gestational exposure ranged from 2 days to 19 weeks and 5 days gestation with the mean gestational age of in utero upadacitinib exposure of approximately 5 weeks and 3 days.
Pregnancy outcomes by disease indication are provided in Table 2. There were 43 live births reported: 42 live births without a congenital anomaly and one live birth with a congenital anomaly. Most of the live birth pregnancies were exposed to upadacitinib during the first trimester only with a mean gestational age of in utero upadacitinib exposure of 5 weeks and 5 days. There were two pregnancies with exposure beyond the first trimester, defined as > 13 weeks gestation. One infant (pregnant patient with non-radiographic axial spondyloarthritis) was exposed through 13 weeks and 2 days gestation and one infant (pregnant patient with atopic dermatitis) was exposed to upadacitinib through 19 weeks and 5 days gestation; both resulted in a live birth without congenital anomaly.
Table 2 Summary of pregnancy outcomes with maternal exposure in upadacitinib clinical trialsOf the 43 live births with known outcomes, one infant had a congenital anomaly, and three infants were born either premature or with complications. The live birth with a congenital anomaly was born to a 30-year-old patient in a Crohn’s disease study who was in a state of clinical remission per the Crohn's Disease Activity Index (< 150) at the time of pregnancy. Exposure to upadacitinib was through 4 weeks and 4 days gestation. The patient had anemia and oligohydramnios during pregnancy and no complications during the delivery or postpartum period were reported. The male infant, born premature at 34 weeks and 5 days gestational age, had an atrial septal defect (ASD) diagnosed by an echocardiogram, a low birth weight of 2030 g (approximately ninth percentile based on prematurity [7,8,9,10]), neonatal transient tachypnea, hyperbilirubinemia, and septicemia. There was no family history of ASD and surgery was not required. No follow-up information was provided regarding spontaneous closure of the presumed ASD. Details of the additional three infants born either prematurely or with complications are further described in Table 3.
Table 3 Summary of pregnant patients who delivered an infant preterm or with complications from clinical trial reportsThe 19 pregnancies resulting in a spontaneous abortion occurred in the following indications: rheumatoid arthritis (13), atopic dermatitis (2), Crohn’s disease (2), ulcerative colitis (1), and psoriatic arthritis (1). Nine patients were taking concomitant methotrexate, a known abortifacient and allowed in some studies, at the time of awareness of the pregnancy. Of the ten patients without background methotrexate exposure, seven had other risk factors for spontaneous abortion, including advanced maternal age [> 35 years] (n = 4), type 1 diabetes mellitus (n = 1), and prior spontaneous abortion (n = 2). Overall, gestational exposure to upadacitinib among all patients experiencing spontaneous abortion occurred prior to 12 weeks gestation (mean exposure: 5 weeks and 2 days). Data on the timing of spontaneous abortions were limited, but for those with available information (n = 10), the median was approximately 8 weeks gestation.
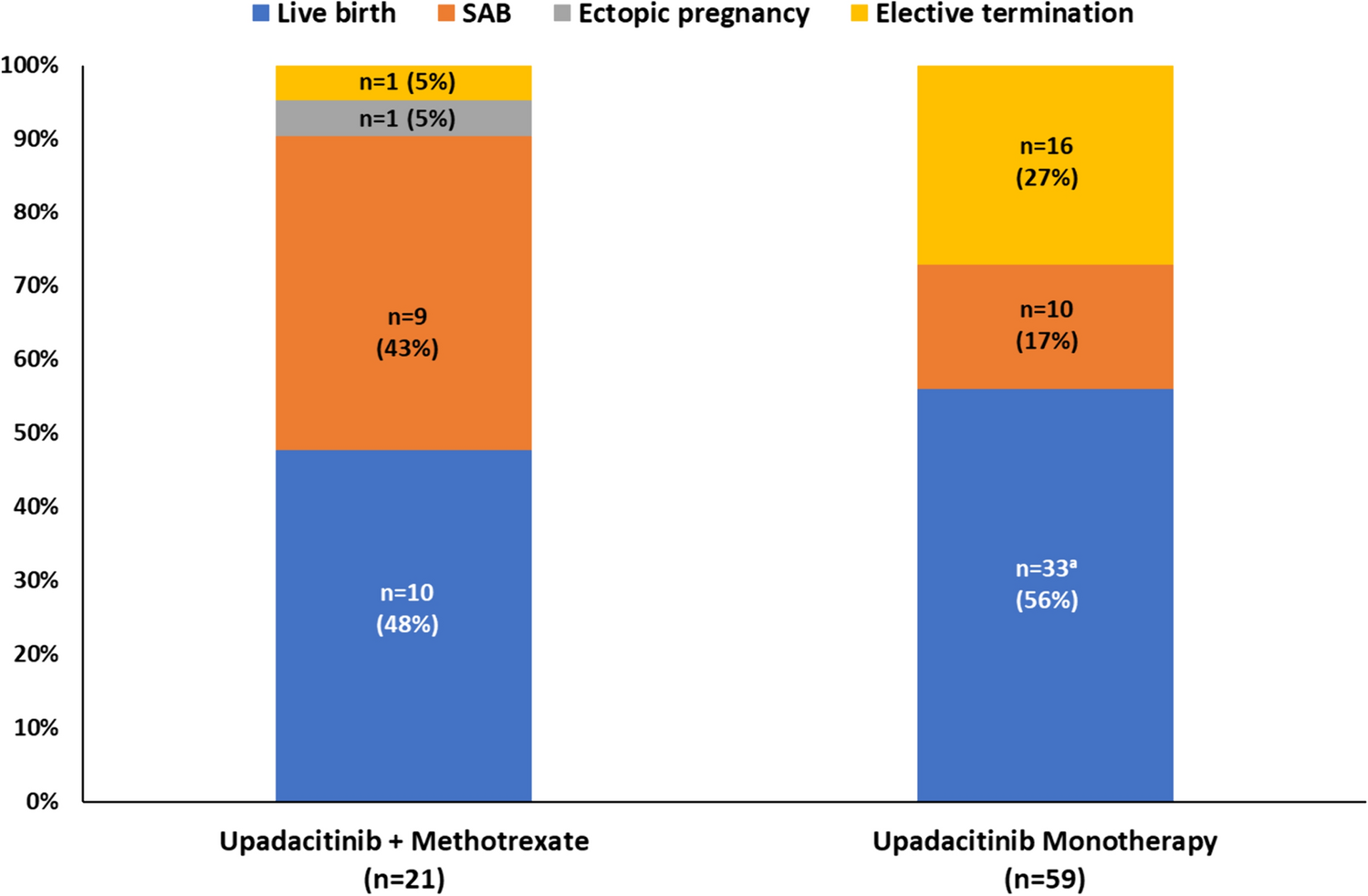
Given the potential fetotoxic effects of methotrexate, further analysis was performed wherein patients were stratified based on the use of upadacitinib monotherapy versus upadacitinib with concomitant methotrexate in the upadacitinib clinical trials. Fifty-nine pregnancies occurred in patients receiving upadacitinib monotherapy, while 21 pregnancies occurred in patients receiving upadacitinib and methotrexate. Pregnancies on upadacitinib with concomitant methotrexate occurred in studies of patients with rheumatoid arthritis (n = 19) or psoriatic arthritis (n = 2). Overall outcomes of these pregnancies, stratified by upadacitinib monotherapy and upadacitinib with concomitant methotrexate, are provided in Fig. 1. Among 59 pregnancies reported in patients receiving upadacitinib monotherapy, there were 32 (54%) live births without a congenital anomaly, 1 (2%) live birth with a congenital anomaly, 10 (17%) spontaneous abortions, and 16 (27%) elective terminations. Among 21 patients receiving upadacitinib with concomitant methotrexate, there were 10 (48%) live births without a congenital anomaly, 9 (43%) spontaneous abortions, 1 (5%) ectopic pregnancy, and 1 (5%) elective termination. There were no live births with a congenital anomaly in the upadacitinib with concomitant methotrexate group.
Fig. 1
Pregnancy outcomes with maternal exposure in upadacitinib clinical trials stratified by concomitant methotrexate use. aIncludes one infant born with a congenital anomaly (atrial septal defect). SAB spontaneous abortion
There were 17 elective terminations and none that reported fetal defects. The reasons provided for the elective terminations were mostly for family planning purposes and few were because of concerns of teratogenicity. One ectopic pregnancy occurred in a patient with psoriatic arthritis; this pregnancy occurred in the context of an intrauterine device, concomitant methotrexate use, and advanced maternal age of 40 years.
A breakdown of pregnancy outcomes by upadacitinib dose is presented in Table S4 in the ESM. Forty-five patients received upadacitinib 15 mg once daily and 31 received upadacitinib 30 mg once daily at the time of the positive pregnancy test. Four patients were on 6 mg twice daily, 12 mg twice daily, or 24 mg once daily and no patients were on upadacitinib 45 mg. Outcomes varied when stratified by dose with no clear patterns observed.
3.2 Postmarketing Pregnancy Cases and OutcomesPostmarketing cases are voluntarily reported and, although proper diligence is performed by AbbVie to obtain the necessary follow-up, postmarketing cases often have missing or no information. Therefore, these cases are discussed separately from the clinical trial reports.
The cumulative total pregnancies reported via postmarketing surveillance was 211, in which there were 159 with unknown pregnancy outcomes and 52 pregnancies with known outcomes. Of the reports with known outcomes, a medical review revealed four pregnancy reports that described discontinuation of upadacitinib prior to pregnancy. These four unexposed pregnancies in addition to cases with unknown outcomes/ongoing at the time of data cutoff (163/211; 77%) were excluded from subsequent analyses.
In the 48 cases of known outcomes with maternal upadacitinib exposure, the majority were reported during treatment for rheumatoid arthritis (n = 26). This is not surprising as the rheumatoid arthritis indication received the first marketing authorization for use of upadacitinib in 2019. The remaining cases were reported during treatment for psoriatic arthritis (n = 2), ankylosing spondylitis (n = 1), atopic dermatitis (n = 3), ulcerative colitis (n = 2), and unknown indication(s) (n = 14). Fourteen cases were prospective (of which 11 are medically confirmed) and 34 were reported retrospectively. Based on the limited number of prospective and medically confirmed cases, prospective and retrospective cases were combined to present the totality of the data. Exposure timing to upadacitinib during gestation was not uniformly collected and missing in some cases; therefore, the exact weeks/days of gestational exposure could not be determined. However, the vast majority reported maternal exposure to upadacitinib was during the first trimester (n = 32) with only a few cases of unknown exposure timing (n = 16).
Postmarketing cases with known outcomes and exposure to upadacitinib (n = 48), composed of live births (22/48; 46%), spontaneous abortions (18/48; 38%), elective terminations (7/48; 15%), and ectopic pregnancy (1/48; 2%) are described here. Twenty-two live births without a congenital anomaly were reported, of which the majority were full term and had no neonatal complications. There were three premature infants (defined as <37 weeks gestation) and one infant of unknown gestational age considered large for gestational age. Further details on these four infants are provided in Table S5 of the ESM.
Eighteen (38%) spontaneous abortions were reported in patients with the following indications: rheumatoid arthritis (n = 13), atopic dermatitis (n = 1), ulcerative colitis (n = 1), psoriatic arthritis (n = 1), and unknown (n = 2). Risk factors reported that could have contributed to a miscarriage were as follows (some patients had multiple risk factors): five patients were of advanced maternal age at ≥ 35 years (three in the early 40s), two on concomitant methotrexate, three with current smoking history, one with adrenal insufficiency, one with uterine abnormalities, one with a history of prior spontaneous abortions, and eight who had no risk factors reported.
Seven elective terminations were reported, among which no fetal defects were documented. One ectopic pregnancy was reported in a patient with rheumatoid arthritis and no other information was provided.
留言 (0)