This post hoc analysis of a phase 2 study found that ropeginterferon alfa-2b elicited a reduction in HCT values, WBC counts, PLT counts, and JAK2 V617F allele burden in Japanese patients with low-risk PV.
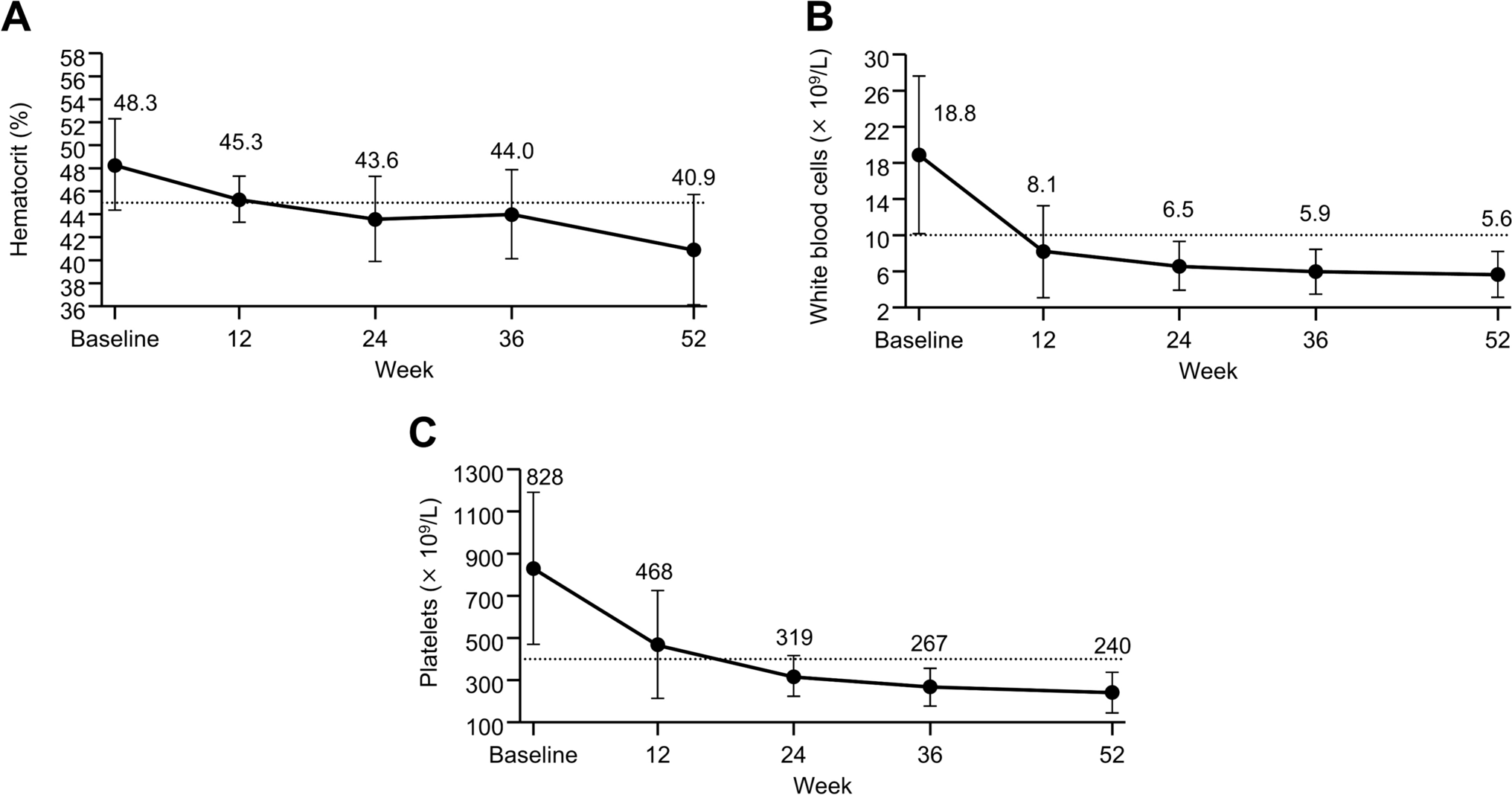
As patients with low-risk PV for whom the standard treatment in Japan is difficult to apply (including patients for whom CRT is recommended because of disease-related signs and symptoms) were enrolled in the original phase 2 study [2, 3, 9], the patients in this analysis exceeded target hematological levels at baseline, and exhibited HCT: 48.3%, WBC: 18.8 × 109/L, and PLT: 828 × 109/L. Lowering HCT levels < 45% is recommended to prevent TEs [4], and elevated WBC and PLT counts are also risk factors for TEs [5, 6]. At 52 weeks, the mean values reached the target value (HCT: 40.9%, WBC: 5.6 × 109/L, PLT: 240 × 109/L), and no TEs occurred, indicating the usefulness of ropeginterferon alfa-2b in low-risk patients with PV.
In the LOW-PV study (which compared standard treatment [phlebotomy and low-dose aspirin] versus standard treatment plus ropeginterferon alfa-2b for low-risk PV), the percentage of responders (HCT < 45% and no disease progression) at 12 months was 81% in the ropeginterferon alfa-2b group [10]. Furthermore, there were fewer mean phlebotomies per patient-year in the ropeginterferon alfa-2b group (2.9) than the standard treatment group (4.2). The percentage of patients who achieved HCT < 45% in our study (85%) was similar to that of LOW-PV. Similarly, fewer patients required phlebotomies following ropeginterferon alfa-2b treatment, indicating consistent outcomes in the Japanese population.
In this analysis, the mean JAK2 V617F allele burden notably decreased, and the proportion of patients with a ≥ 50% variant allele frequency decreased from 89.5% at baseline to 42.1% following 52 weeks of treatment. Furthermore, no cases experienced myelofibrosis transformation. A previous study found that patients with higher JAK2 V617F burden (> 50% variant allele frequency) have a higher myelofibrosis transformation rate than patients with < 50% frequency [14]. Therefore, the decreased JAK2 V617F allele burden following ropeginterferon alfa-2b treatment may have contributed to a reduced myelofibrosis transformation risk. Younger patients and those with low allele burden are reported to be more likely to have a molecular response to ropeginterferon alfa-2b [8]. Similarly, patients who achieved < 50% allele burden at week 52 had a lower baseline allele burden compared to those who did not (64.4% vs 91.5%) in this study. Additionally, the proportion of patients with CHR at week 52 was 100% (10/10 cases; one case could not be determined due to discontinuation) in patients who achieved < 50% allele burden at week 52. These results suggest that an allele reduction is associated with the CHR achievement. However, longer studies with larger populations are needed to confirm these results and to determine which patients are more likely to achieve a molecular response in Japanese patients with low-risk PV.
Although TEAEs related to ropeginterferon alfa-2b occurred in all patients, no treatment-related grade ≥ 3 TEAEs occurred. As in the original phase 2 study, the most common TEAE was alopecia [9]. One patient who discontinued treatment because of silent thyroiditis related to ropeginterferon alfa-2b had no history of thyroid dysfunction and was positive for anti-thyroid peroxidase antibodies and negative for anti-thyroglobulin antibodies at baseline [13]. Therefore, it is advisable to monitor thyroid function and thyroid antibodies both prior to and following ropeginterferon alfa-2b initiation.
Our results indicate that ropeginterferon alfa-2b can effectively reduce HCT, WBC counts, PLT counts, and JAK2 V617F allele burden, reducing phlebotomy requirements, in Japanese patients with low-risk PV. Although other details (including clinical symptoms, duration, and phlebotomy frequency) were not recorded, and despite a relatively small sample size and short duration, our results support ropeginterferon alfa-2b as a treatment option for patients with low-risk PV who do not respond adequately to phlebotomy and low-dose aspirin.



留言 (0)