Participants
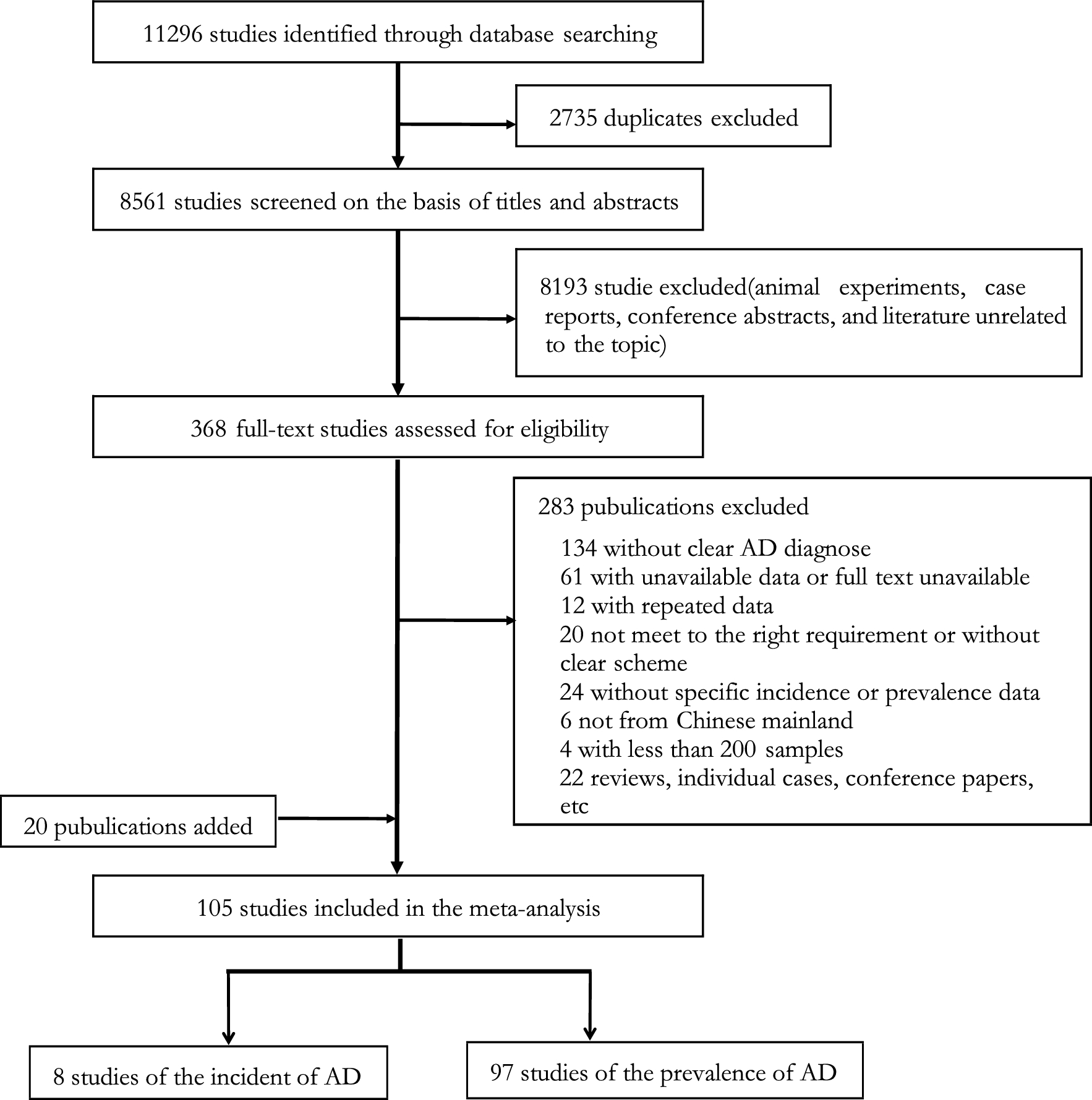
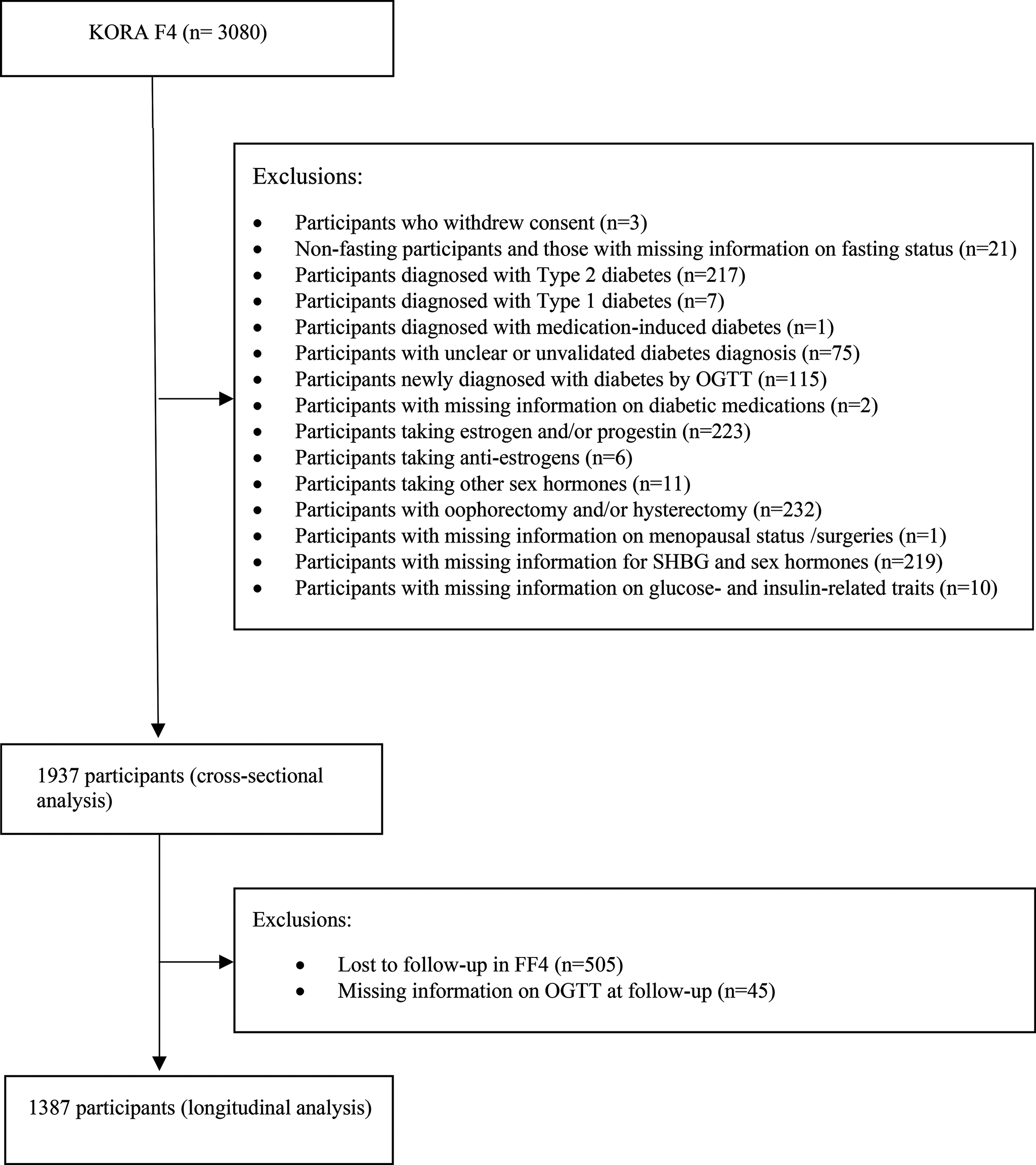
This study was based on data from the Danish Conscription Database (DCD) [15] and the Danish Conscription Registry (DCR) including nearly all Danish men examined at conscription from 1957 to 1984 and 2006–2015, respectively [16]. The data were restricted to men because DCD and DCR only include < 1% women, which are highly selected. Information on the included traits is not available in other Danish registers. The majority of men, especially in DCD, were ethnic Danes. There was a gap in the registration and digitalization of information collected at the Danish conscriptions in the period 1985–2005. In Denmark, all men are requested by law to appear before the conscription board for a health examination between the ages of 18 and 26 years. We linked these data through the Danish national identification number, assigned to everyone living in Denmark since 1968, with the Danish Civil Registration System, the Danish Psychiatric Central Register, the Danish National Patient Registry, and the Danish Cause of Death Registry (Supplementary Fig. 1). The initial study population included 1,092,823 men from DCD and DCR as described in Supplementary Fig. 2. Due to exclusion of 132,151 men with missing information, 8,545 men not in the birth cohort 1939-59 for DCD or not in the age range 18–30 years at the time of conscription, 13,458 females and 750 who were inactive in the CPR register, the study population at risk of death included 937,919 men. Among men excluded from the study due to missing information, the majority had been exempted from the conscription examination due to medical conditions such as mental retardation and other psychiatric conditions, asthma, epilepsy, or type 1 diabetes, however, the specific cause was not available in the register. After exclusion of 564 men with schizophrenia at baseline, the study population at risk of schizophrenia included 937,355 men, and after further exclusion of 285,551 men without measures of BMI, a sub-study population with measures of BMI included 652,368 men (Supplementary Fig. 2). In previous a paper, we have shown that men with missing information on BMI do not represent a selective part of the study population [12]. This information has been added to Supplementary Fig. 2.
The study was approved by the Danish Data Protection Agency. All data were retrieved from administrative registers, which according to Danish law implies that informed consent was not required of participants.
Measures
The selected traits were measured by cognitive ability, educational duration, height, and body mass index (BMI) in young adulthood identified in DCD and DCR.
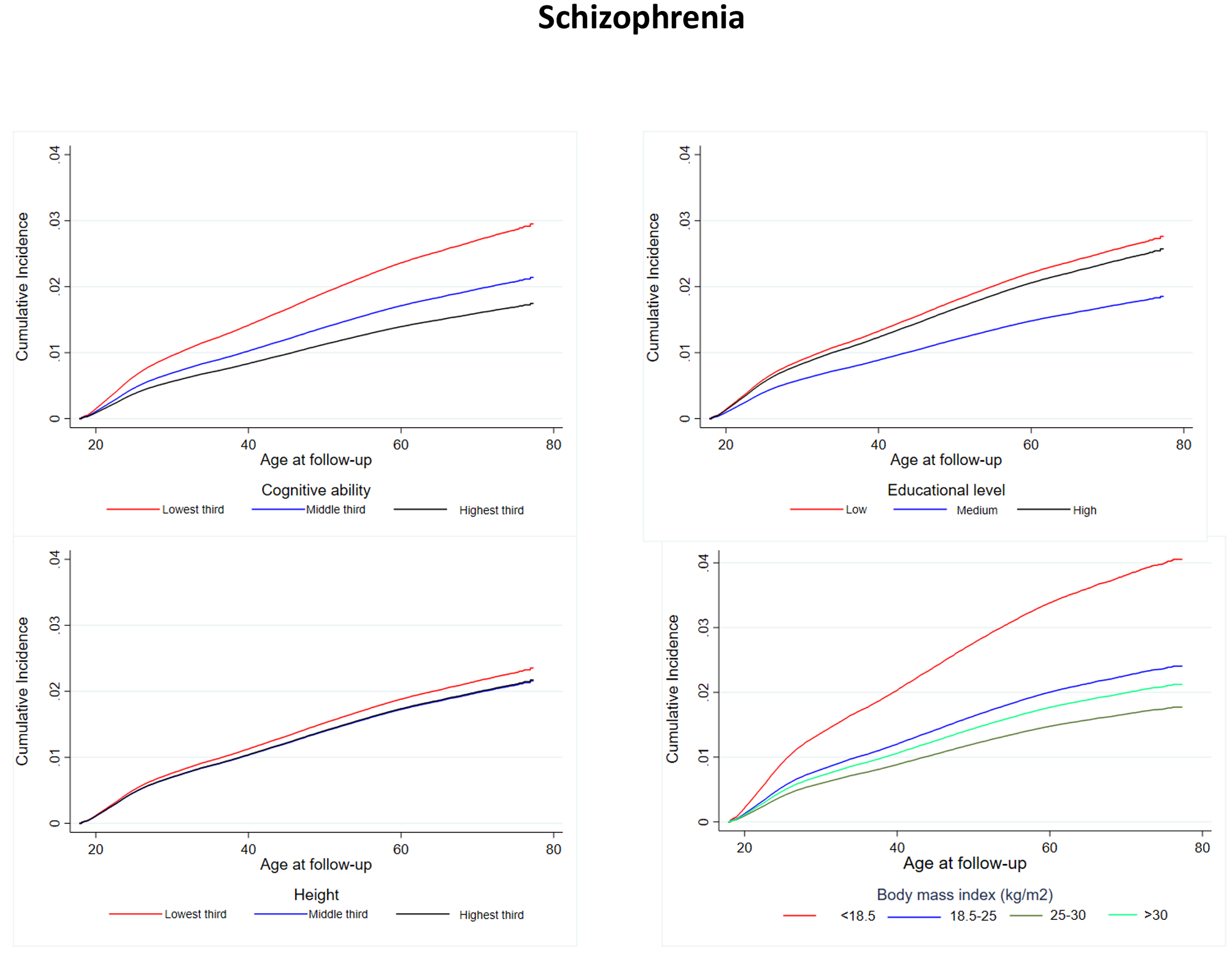
Cognitive ability was assessed by the conscription intelligence test called the ‘Børge Prien Prøve’ (BPP), which comprises logical, verbal, numerical, and spatial subtests. The BPP score ranges from 0 to 78 and correlates well with the full-scale Wechsler Adult Intelligence Scale IQ score (r = 0.82) [17]. Cognitive ability was investigated by tertiles of birth cohort-specific z-scores. Information on the educational duration reported at conscription was categorized into low (7th -9th grade), medium (vocational training or 10th -11th grade), and high education (12th grade or more advanced).
Information on the height and weight measured at the conscription examination was retrieved from the DCD and DCR databases. Height was measured without shoes and weight was measured wearing only underwear. Height was investigated as tertiles of birth-specific z-scores and BMI (kg/m2) was divided into: (i) underweight:<18.5 kg/m2, (ii) normal weight:18.5 to < 25 kg/m2, (iii) overweight:25 to < 30 kg/m2, and (iv) obese:>=30 kg/m2 [18]. The lowest tertile of cognitive ability and height and shortest education, respectively, were used as reference to illustrate the possible linear associations. For BMI, normal weight was used as reference category to follow the suggestions by WHO.
Schizophrenia
Using the person identification number as a key, schizophrenia was ascertained by the linkage with the Danish Psychiatric Central Register and the Danish National Patient Registry as the first discharge diagnosis from a psychiatric or somatic ward until the end of follow-up (31st of December 2014) [19]. The registers hold individual-level data on the type of patient contact (inpatient information from 1969 to 1977, respectively; emergency room and outpatient information from 1995), discharge diagnosis, and date of admission and discharge for all hospital admissions in Denmark. Diagnoses have been coded according to the 8th Revision of the International Classification of Diseases (ICD-8) from 1969 to 1994, and the 10th Revision (ICD-10) from 1995 and onwards. Schizophrenia was identified by ICD-8: 8:295.x9, 297.x9, 298.29-298.99, 299.04,299.05, 299.09; and ICD-10:F20-F29. ICD-9 was not used in Denmark. There exists a relatively good concordance between the codes used for schizophrenia in ICD-8 and ICD-10 and we used the approach used in previous Danish studies [20].
Vital status and causes of mortality
Information on the time of emigration and death was obtained from the Danish Civil Registration System. Information on mortality from natural and unnatural causes was retrieved from the Danish Cause of Death Registry from 1st of January 1970 until 31st of December 2014. Mode of death and specific primary cause of death were used to identify death from unnatural causes. Death from unnatural causes was defined by death of suicide, homicide accidents, and other external causes in the International Statistical Classification of Disease, injury and cause of death. Death from natural causes comprised all other deaths.
Statistical analysis
In the analytical models with schizophrenia as the outcome, the men were followed from their age on January 1st, 1969 (the date the Danish Psychiatric Central Register was initiated) or date of conscription examination, whichever came last, and until the first registration of a schizophrenia diagnosis, emigration, death or end of follow-up (31st of December 2014), whichever came first. The analytical models for mortality outcomes followed men from April 1st, 1968 (the date the Danish Civil Registration System was initiated) or date of conscription examination, whichever came last, and until the first registration of emigration, death, or end of follow-up (31st of December 2014), whichever came first. Age was the underlying time scale of the models and thus, automatically accounted for.
Nelson-Aalen cumulative hazard curves of schizophrenia, death from natural causes, and death from unnatural causes were calculated taking competing risk of death and death from other causes into account as censoring events. The analyses were stratified by each of the four traits (cognitive ability, educational duration, height, and BMI). The competing risk analysis is not appropriate for time-varying exposures (in this case schizophrenia). Thus, for the competing risk analyses of death from natural and unnatural causes, respectively, comparisons were based on men with schizophrenia and a time-matched reference population. The reference population was randomly selected among members in the cohort who had remained free from schizophrenia at the time of matching and who had reached the same age as the case in a 1:5 ratio (n = 73,872). Individuals in the reference group were censored if they were diagnosed with schizophrenia (n = 517).
To estimate caseloads rather than relative hazards estimated by the usual Cox regression model, we used Aalen’s additive hazard model [21]. It was first applied to estimate additional incident cases of schizophrenia per 100,000 person-years (py) associated with the traits (young adult cognitive ability, educational duration, height, and BMI). Secondly, the model was used to estimate additional cases of death from natural and unnatural causes, respectively, per 100,000 py associated with the traits including interaction terms with schizophrenia. The assumption of the time-constant hazard difference of this additive model was assessed graphically by the cumulative coefficient vs. time plots. The analyses of the traits cognitive ability, educational duration, and height of young adults were conducted with mutual adjustment for the other traits (young adult cognitive ability, educational duration, height). Furthermore, the multiple adjusted analyses of BMI in the sub-study population were also adjusted for young adult cognitive ability, educational duration, and height. All analyses were stratified on birth cohort in seven categories (1939–1944, 1945–1949, 1950–1954, 1955–1959 for the DCD cohort, and 1985–1989, 1990–1994, 1995–1997 for the DCR cohort). Interactions between schizophrenia and each of the traits measured in early life were investigated by including interaction terms in the models of death by natural and unnatural causes, respectively.
In supplementary analyses, separate additive hazard regression analyses for the DCD and the DCR cohort were conducted to identify possible cohort differences. For these analyses, the DCD cohort was restricted to the birth cohorts 1950–1959 and followed from their conscription examination until 1978-80 to ensure comparable follow-up time in the two cohorts. Also, to account for the possible confounding impact of the father’s social status measured by highest earned education, supplementary analyses for the DCR cohort with adjustment for the father’s educational duration were conducted.
Due to multiple testing of the main analyses (21 test based on 4 (cognitive ability, educational duration, height and BMI), 3 outcome (schizophrenia, death from natural and unnatural causes, respectively) and additionally 9 tests of interaction, we applied Bonferroni corrections and divided the confidence interval with 21. Thus, we used a significance level of 0.24% instead of 5% and calculated 99.76% (from now 99%) confidence intervals for the main analyses.
All analyses were performed in Stata-15 and the statistical software program R.

留言 (0)