This study examines three external causes of death that are differentiated by intention. These three categories are: Intentional injury deaths, unintentional injury deaths, and undetermined/ill-defined deaths. These followed the definition set out in the WHO Mortality Database, with intentional injury deaths referring to suicide deaths (ICD-10 codes: X60-X84, Y870) – called “suicides” hereafter. Unintentional injury deaths include all kind of accidents (e.g. car accidents) and accidental poisoning – either by medication or alcohol/illegal substances. Hereafter, the former are referred to as “accidents” (V01-X32, X40, X43, X46-X59, Y40-Y86, Y88, Y89, U12.9) and the latter – deaths due to illegal substances and alcohol – as “drug use disorder deaths” (F10-F16, F18-F19, X41-X42, X44, X45). Deaths of undetermined intent (Y10-Y34, Y872) are those, where it is not possible to know whether the death of a person was intentional or not. These include cases of death, in which it remains unclear whether an injury death, as described above, was a suicide or an accident. We also include ill-defined deaths (R00-R94, R96-R99) – these are deaths, where the death certification procedure did not find a specific cause of death (e.g. unattended deaths, death not otherwise specified). Note that the WHO classification of ICD-10 codes provides a set of mutually exclusive categories [16]. In that WHO classification system drug use disorder deaths should not be confused drug poisoning. These are categorized by the WHO into a number of categories, of which the following are relevant for this analysis: “Suicides” (i.e., ICD-10, X60–X69: intentional self-poisoning), “Accidents” (i.e., ICD-10, X40, X43, X46-X49: accidental poisoning), “Deaths of undetermined intent” (i.e., ICD-10, Y10–Y19: poisoning with undetermined intent) and drug use disorder deaths (i.e., ICD-10, X41–X42, X44–X45: accidental drug poisoning not elsewhere classified). Evidently, drug poisoning—as the mechanism of dying – underpins all categories. More precisely, a person can use drug poisoning as a means to commit suicide, poison themselves on accident, the poisoning may be of undetermined intent, or fall under a drug use disorder related death.
Consequently, as drug poisoning can be the mechanism of death in all the above-mentioned categories, this makes misclassification between these categories more likely. More specifically, these categories may be mutually exclusive in theory but are often hard to distinguish in practice, due to their shared mechanism.
Data analysis
Data was obtained for the last forty years, i.e. from 1982 until 2022 from the WHO mortality database. Autopsy rates were obtained from the European regional offices’ European Health for All Database (https://gateway.euro.who.int/en), the CDC (https://wonder.cdc.gov/) and Statistics Canada (https://www.statcan.gc.ca/en/start). For sensitivity analyses, additional indicators were retrieved from the OECD (https://data-explorer.oecd.org/). To improve robustness, individual years were averaged into periods: For the longitudinal analysis, eight five-year periods, starting with 1982–86, were calculated. For cross-sectional analysis, four ten-year periods, starting with 1982–91, were calculated.
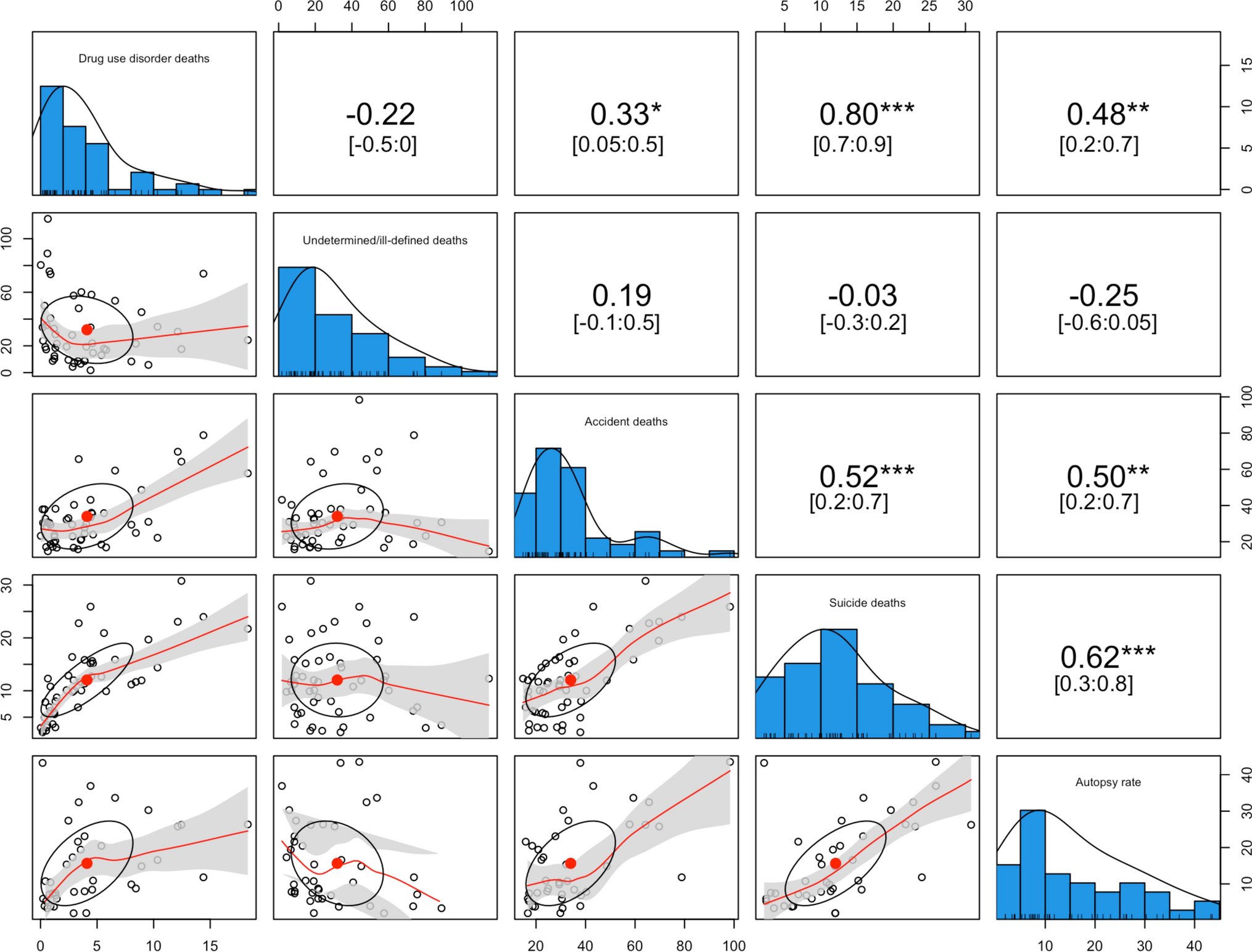
For the cross-sectional analysis we conducted spearman correlations, bivariate regressions, and multiple regressions. The regressions were used to investigate the associations of each aforementioned variable with suicide and accident deaths.
Longitudinal data analysis was conducted using generalized estimating equations (GEEs). First, we implemented crude models and then two multiple GEEs were calculated. Similar to the regression models, the GEEs were calculated in order to investigate the associations of each aforementioned variable with both suicide and accidents.
The formula of both of the multiple regression models and of the multiple GEEs used identity links and a gamma distribution and can be described as following: For the model predicting suicides (per 100.000), the predictors were autopsies (per 100 deaths), drug use disorder deaths (per 100.000), undetermined/ill-defined deaths (per 100.000), and accidents (per 100.000). That is to say: Y(suicides)i = β0 + β1 accidents1i + β2 drug use disorders deaths + β3 undetermined/ill-defined deaths3i + β4 autopsy4i + εi). For the model predicting accidents, the predictors were autopsy rates, drug use disorder deaths, undetermined/ill-defined deaths, and suicides (i.e. Y(accidents)i = β0 + β1 suicides1i + β2 drug use disorder deaths2i + β3 undetermined/ill-defined deaths 3i + β4 autopsy4i + εi). Thereby, Y is defined as μ, the mean of the outcome Y, moreover μ is transformed using the identity link: 1/μ. The inclusion of time as an additional predictor to the above-mentioned variables was specific to the longitudinal model.
As accidents and suicides were non-negative and right skewed, gamma distributions were used for both the regression models and GEEs. The correlation structure of the longitudinal model was chosen based on quasi-likelihood under the independence model criterions (QICs) [17].
Sensitivity analysis
Sensitivity analyses were undertaken to investigate the robustness of results. We investigated (a) data quality, (b) indicator specification and (c) the impact of antidepressant use. Data quality was investigated in two ways: First by limiting countries to only EU member states, and second by only including countries with high data quality according to the WHO data quality classification (https://platform.who.int/mortality/about/data-quality). The impact of indicator specifications was investigated by dividing both undetermined/ill-defined deaths and drug use disorders deaths into their subcategories (ill-defined diseases and ill-defined injuries, and illicit drug use disorder deaths and alcohol use disorder deaths). The effect of antidepressants was investigated by including defined daily doses, reported on the national level and provided by the OECD, into the aforementioned models. All analysis was conducted using R version 4.3.2 [18]. This analysis was preregistered on OSF before data retrieval, under: https://osf.io/8pgst.





留言 (0)