Most myelolipomas have no clinical symptoms. Most of them are accidentally found during physical examination or imaging examination due to other diseases [4]. In addition, in most patients, mediastinal myelolipoma appears around the age of 60, and there has been no significant relationship reported between gender and tumors [5, 6]. Similarly, in our study, the highest incidence rate was approximately 60 years old. However, we found that the incidence rate in males was significantly higher than that of in females. This was inconsistent with previous studies and may have been related to the fewer cases and statistical errors in previous studies.
Mediastinum accounts for approximately 3% of all myelolipomas and is mainly located in the lower right posterior mediastinum [5]. In our study, 68.4% of the cases were located in the right posterior mediastinum. Mediastinal myelolipoma can be single or multiple and located on one or both sides of the posterior mediastinum [7, 8]. In rare cases, it has been located in the anterior mediastinum; however, the study did not mention the image features [9]. In our study, most cases were unilateral lesions and 26.9% of the cases were bilateral lesions.
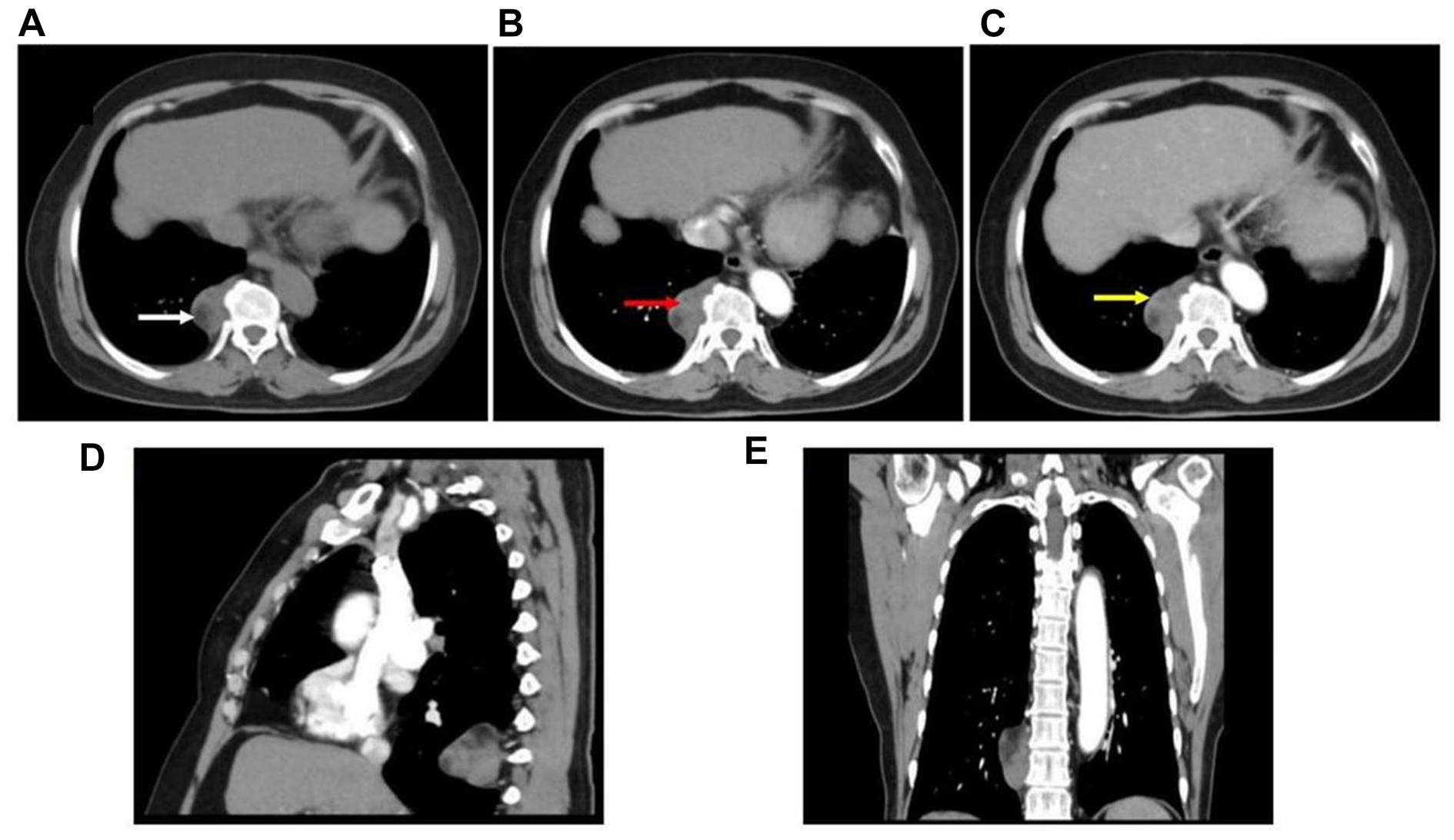
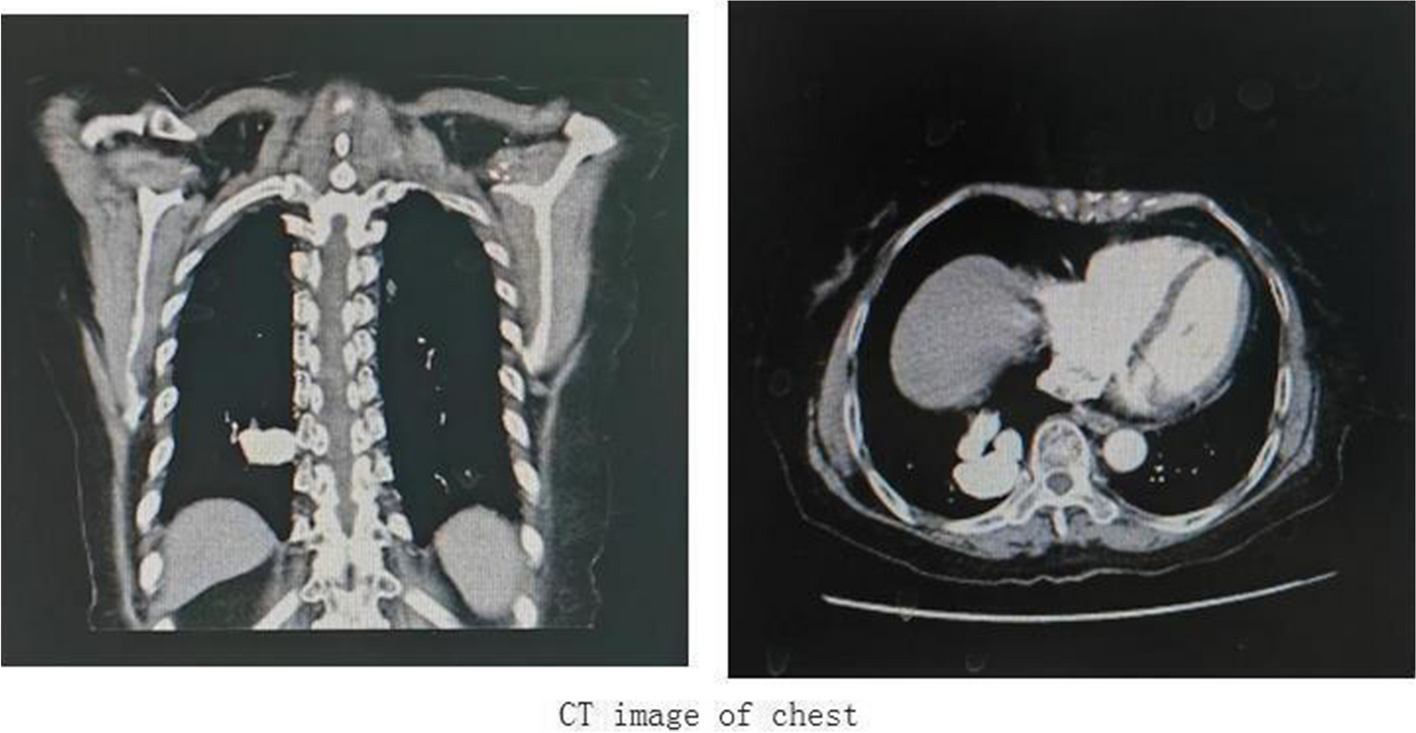
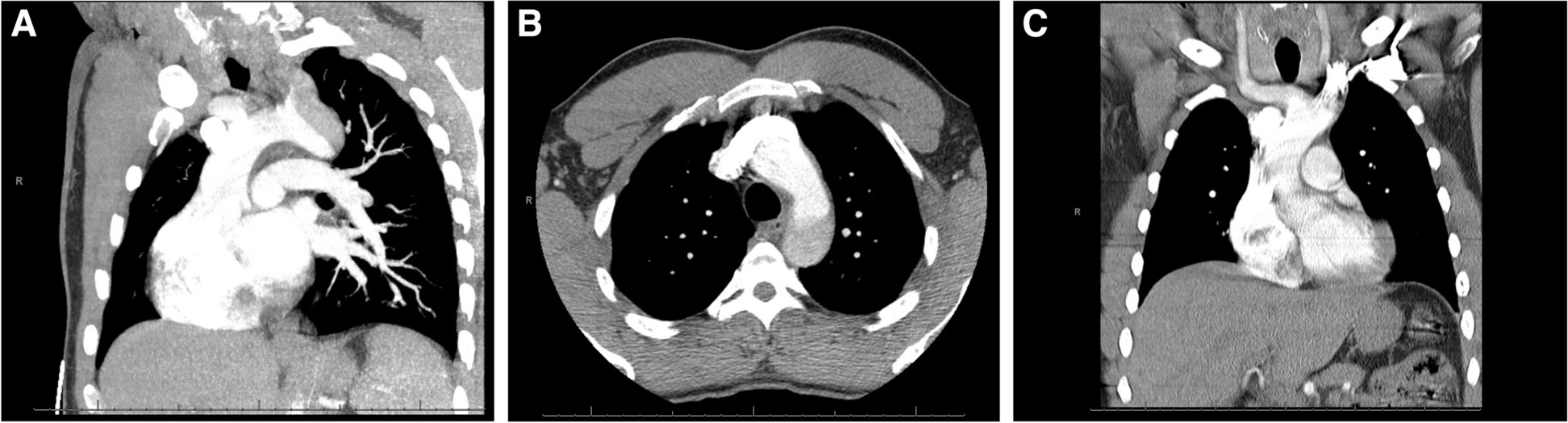
According to one study, the CT value of the tumor, which included fat and bone marrow tissue, was 20–50 Hu. In the case of the contrast agent, tumor enhancement was not obvious. In addition, calcification in tumors is rare [10]. This is roughly consistent with our study. In our study, fat-like density could be seen in most lesions (84.8%). After contrast enhancement, most lesions (93.9%) had mild to moderate enhancement, and only a few lesions (12.1%) showed calcification. Most lesions were heterogeneous and encapsulated.
There is little information on MRI-related reports of mediastinal myelolipoma. Because tumors contain fat components, most tumors have high signal intensity on T1WI and T2WI [11]. According to the main content of the mass, MRI may show equal intensity or slightly higher intensity in T1- and T2-weighted images [6]. One researcher mentioned that the MRI signal of mediastinal myelolipoma could be divided into three types according to the tumor components: fat signal, adult cortex signal, and signal between fat and liver [12].
CT is a common diagnostic method for mediastinal myelolipoma. CT and MRI can effectively diagnose adrenal myelolipoma, but they cannot diagnose mediastinal myelolipoma [13]. Even if the disease cannot be accurately diagnosed, it can be judged whether the disease is benign or malignant by using imaging [11]. Different tumors can be distinguished by their occurrence in distinct locations and the different tissue components present within a tumor. In particular, mediastinal myelolipoma needs to be differentiated from teratoma, neurofibroma, schwannoma, malignant nonseminomatous germ cell tumors, thymolipoma, angiolipoma, and epidural lipomatosis [14].
Adrenal myelolipoma is relatively common. It often occurs unilaterally, with a small volume, clear boundary, circular homogeneous mass, and often contains fat [15, 16]. It is notable that the amount of fat is much less in mediastinal myelipoma than in adrenal myelipoma.
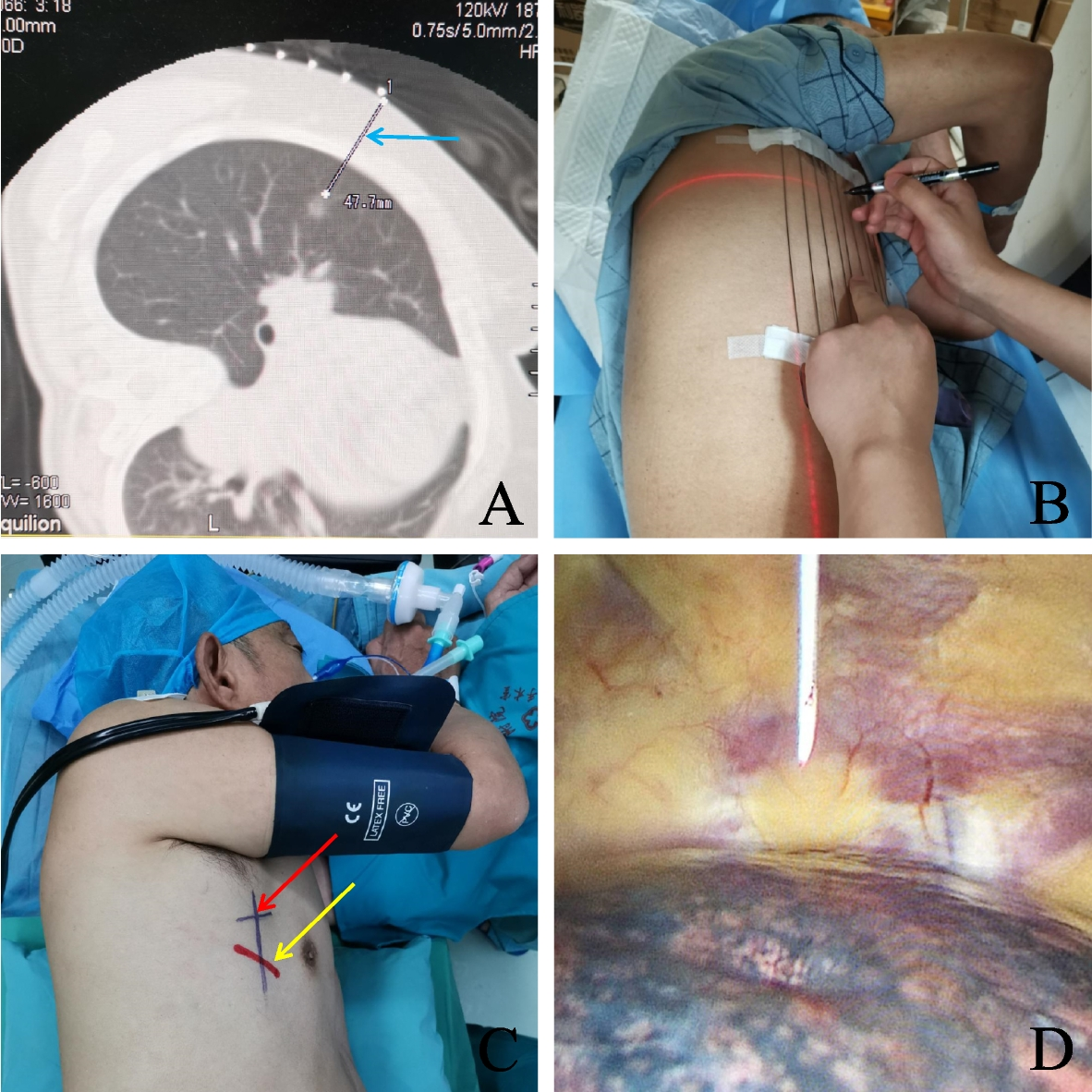
When a paraspinal posterior mediastinal mass is found, especially if the mass is located in the right posterior mediastinum, in addition to the clear boundary and regular shape of the benign tumor signs, if the mass contains fat density, the possibility of myelolipoma should be considered first. Except for special situation such as extremely large masses, internal bleeding, and compression symptoms, radiologists should recommend follow-up rather than biopsy or surgery [17, 18].
General laboratory tests for myelolipoma show no abnormalities, and CT and MRI are the most important preoperative diagnostic methods; CT is more commonly used than MRI. In this study, some radiographic signs were characteristic, with the main radiographic sign being a heterogeneous mass in the right posterior mediastinum near the spine, including fat density. When the imaging features of the lesions are not typical, they mainly need to be differentiated from neurogenic tumors, extramedullary hematopoiesis, lymphadenopathy, and pleural mesothelioma.

留言 (0)