
記住我





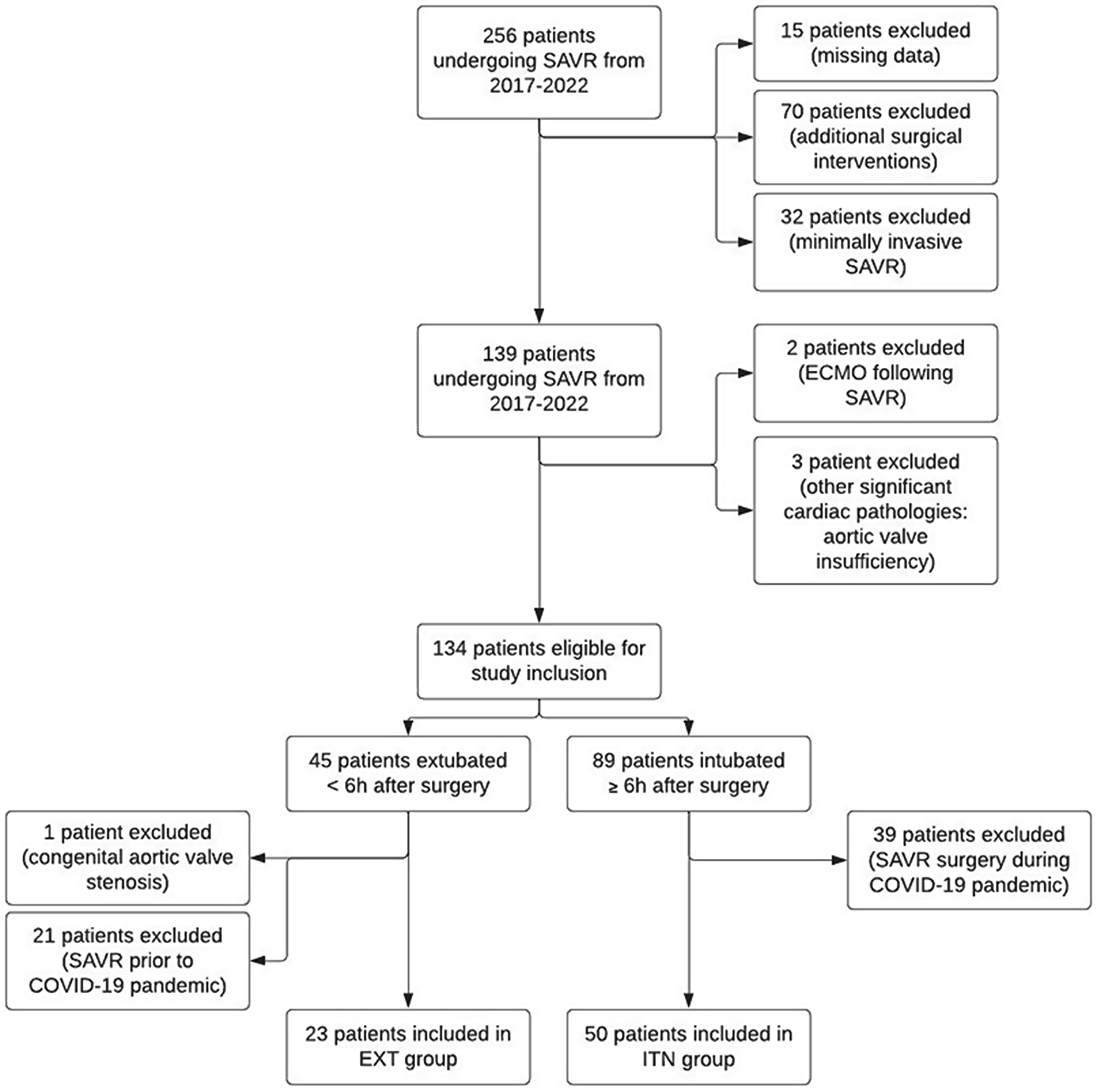
We conducted a multi-center, prospective, parallel group, randomized, controlled trial enrolling patients after thoracic procedures in which visceral pleura remained intact at the end of surgery between August 2020 and September 2023. These procedures did not involve the lung itself, therefore the visceral pleura was not breached. After completion of the procedure a suction seal test (SST) [3] was conducted on all patients. If suction-seal test was positive to confirm absence of air leak, patients were randomized to either receive low auto-suction drain as a solo pleural drain (drainage group) or not to receive drain (drainless group) (Fig. 1). We excluded patients who had chest wall resection (> 2 ribs), accidental major hemorrhage, dense pleural adhesions, redo procedures, or removal of large mediastinal masses (defined as any mediastinal mass that cause mechanical compression of vital mediastinal structures due to the sheer weight and volume of the tumor).
Fig. 1
Pathway, randomization, and results of 111 patients included in the study. CXR: chest x-ray, Pnx: pneumothorax, PL: pleural effusion, SE: surgical emphysema, POD: postoperative day, OPD: outpatient department
Thoracoscopic dataWhenever the VATS approach was indicated, we used KARL STORZ endoscope with 30-degree camera. For patients with pleural biopsy, we used the Uniport technique. A 2 cm skin incision was performed in the planned intercostal space and the parietal pleura was opened under direct vision. The index finger was used to lyse the possible adhesions of the lung to the chest wall, and the trocar was always inserted by means of a Kelly clamp [6].
Confirmation of absence of air leak and sealed woundAfter confirming that there was no air leakage from the treated lung evident by visual inspection of any visceral pleural breach and negative bubble test if needed. We conducted a suction seat test (SST) [3] to test for air leak either from around the drain site (i.e. unsealed system) or incidentally disintegrated visceral pleural surface. A 10 F Redivac tube was tunneled for at least one intercostal space above or below the incision level to create a valve mechanism. This tube was then connected to 250 ml bottle while the knob was deflated, and the tube remained clamped. After closing all the incisions and painting them with Dermabond skin glue, the clamps were released. The SST test is considered positive (i.e. no air leak) if the knob/container remains deflated. On the other hand, if it fails to maintain suction by inflated knob or inflate after collapse, the test is considered negative (i.e. presence of air leak or unsealed system). A negative test was conducted one more time after exclusion of unsealed system by ensuring tight entry wound, sealed connectors, and uncracked tubes. In the drainage group, the 10 F Hemovac drain was left in situ after ensuring adequate tunneling as the drain should be inserted through the same incision but undermined to a higher or lower intercostal space to create valve mechanism. This tightens the wound closure at the drain exit of the chest wall. This track can be done submuscular or subcutaneously. In the drainless group, the drain was removed, and the site was closed tightly and efficiently to ensure sealed wounds.
RandomizationAfter confirmation of absence of air leak and sealed wound, Patients were randomized at a 1:1 ratio according to the patient number in the study. Patients were assigned to either the drainless or drainage group according to the sequence of patient enrolment in the study. Odd numbers were assigned to drainless group and even numbers were assigned to low suction drain.
Postoperative monitoring and care after surgeryAll patients were extubated in the operating theater and managed according to the same protocol. Postoperatively, patients were transferred to a recovery unit for a few hours and subsequently to the thoracic surgical ward. Chest X-ray (CXR) was performed at 4 to 6 h after procedure and on postoperative day 1 (POD1). We define pnx less than 5 cm as “Small pnx” and effusion that did not exceed the shadow of the 6th rib anteriorly as “Minimal effusion”. In the drainage group, the suction-seal and amount of drainage was hourly documented during the first 4 h after the operation. Thereafter and up until drain removal, the chest drain was checked at least once in every shift, three shifts per 24 h. This continuous evaluation by the surgical team aimed to early detection of suction failure and help with early decision to swap to one way valve such as underwater seal drain if suction cannot be maintained. On the surgical ward all patients followed a routine postoperative course, including checking air entry, surgical emphysema, and pain, wound, blood, antibiotic, and comorbidities management. In addition to physiotherapy and nutritional support. Drains were removed if the CXR was deemed satisfactory by primary surgeon after an independent official report of no significant Pnx or PL.
In the drainless group, CXR were performed at 4 to 6 h after procedure and repeated on postoperative day 1 (POD1). The size of residual pneumothorax was defined as the largest distance between the pleural line and the chest wall on CXR. Patients were eligible for discharge if no notable pneumothorax (less than 5 cm in diameter) was noted on serial CXR.
All patients were seen at the outpatient clinic a week after the procedure. Repeat chest x-ray was not required if breath sounds were normal on auscultation unless partial pneumothorax or pleural effusion was detected on postoperative CXR. If any radiological but clinically insignificant abnormalities were detected, a second review in two weeks’ time to follow the patients’ progression was planned.
Statistical analysisthe outcomes of the randomly assigned 100 patients were analyzed. Continuous variables are expressed as means ± SD and compared using t tests. Categorical variables are expressed as percentages and were compared using Pearson chi-square tests. Statistical analyses were performed using SAS software (version 21, IBM, Armonk, NY).
留言 (0)