Study population
This prospective study enrolled 57 healthy adult volunteers at the First Affiliated Hospital of Anhui Medical University between July and September 2023. All participants provided written informed consent, and the institutional ethics committee approved the study protocol. Volunteers were consecutively recruited and comprised 18 males (mean age 26.4 ± 6.7 years) and 39 females (mean age 25.9 ± 6.6 years). To ensure volunteers were eligible for the study, all participants underwent a comprehensive health assessment prior to enrollment. This included: (1) Medical history questionnaire to screen for any pre-existing cardiovascular conditions, risk factors, or other relevant diseases. (2) Physical examination by a study physician, including heart auscultation, blood pressure measurement, and assessment for any concerning signs or symptoms. (3) A 12-lead electrocardiogram (ECG) was obtained and reviewed by a cardiologist to rule out any conduction abnormalities or other ECG findings that could indicate underlying heart disease. Only volunteers confirmed to be free of any overt cardiovascular disease or related risk factors, with normal screening results on history, exam and ECG, were found eligible and enrolled into the study.
MR imaging protocol
CMR imaging was performed using a 3.0 T clinical scanner (Ingenia 3.0 T CX, Philips Healthcare, Best, the Netherlands) with a 32-element body coil. Subjects were scanned in the supine position with headfirst.
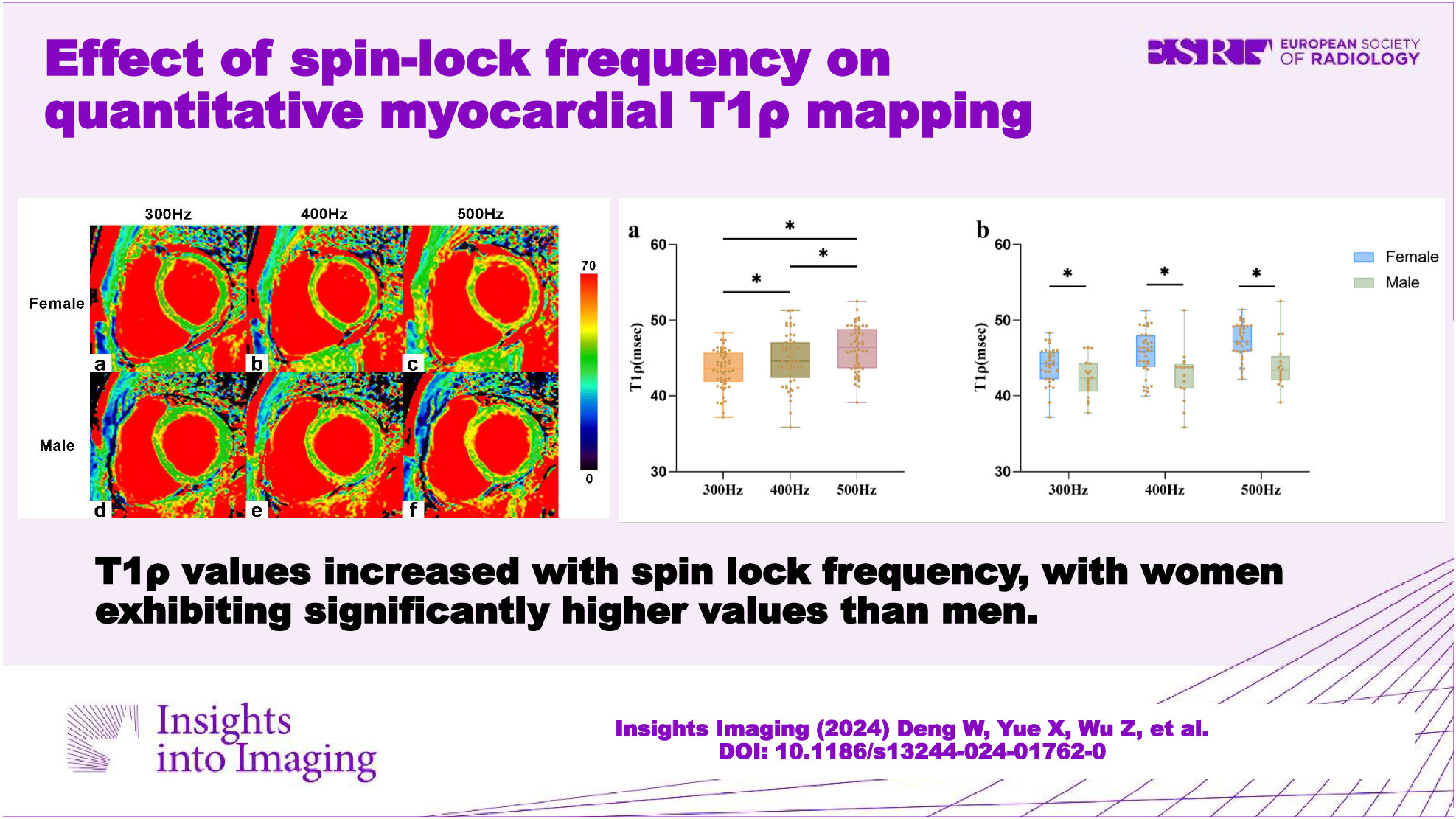
Cardiac gating was achieved using a wireless ECG device (Philips) with four MRI-compatible electrode pads on the left chest. Local B0 shimming optimized field homogeneity over the heart. T1ρ mapping was performed in 3 short-axis slices (basal, mid, and apical) using a T1ρ-prepared balanced steady-state free precession (bSSFP) sequence. Spin-lock pulses of 300 Hz, 400 Hz, and 500 Hz amplitude were applied within scanner-specific absorption rate limits, then nine T1ρ images were acquired per subject. The T1ρ spin-lock frequency order (300 Hz, 400 Hz, 500 Hz) was randomized for each participant. T1ρ maps were generated by fitting spin-lock times of 0, 13.3, 26.6, and 40 msec to a 3-parameter nonlinear least squares model using the Levenberg-Marquardt algorithm [19]. Image acquisition was performed in a single breath-hold per slice, with ECG triggering to minimize cardiac motion artifacts. The pulse sequence repetition time was three heartbeats, providing full slice coverage in 10 heartbeats (around 12 seconds). The T1ρ preparation scheme consisted of 90°x-SLy-180°x-SLy-90°x with refocusing pulses and dual spin-locks with opposite phases for B0/B1 correction [17]. Imaging parameters were: slice thickness 10 mm, matrix 180 × 148, bandwidth 2572 Hz/pixel, TR/TE 1.82/0.71 msec, FOV 360 × 297 mm2, flip angle 35°, SENSE factor 2, NSA 1, shot interval three heartbeats (Table 1).
Table 1 MR imaging parametersTo assess scan-rescan reproducibility, ten volunteers underwent repeat CMR examination after exiting the scanner and resting briefly. Identical imaging protocols were utilized for the initial and repeat scans.
Image processing and data analysis
Four different spin locking durations (TSL = 0, 13.3, 26.6, 40 msec) were used to calculate each T1ρ map using MATLAB (Version R2018b; MathWorks, Natick, MA). A monoexponential two-parameter decay model was applied using a Levenberg–Marquardt algorithm of nonlinear estimation to fit the T1ρ-relaxation time [19], which are described previously [20]. The left ventricular myocardium was divided into 16 segments per American Heart Association standards. Endocardial and epicardial borders were identified automatically and corrected manually. To minimize blood pool and epicardial fat effects, endocardial contours were shifted 10% outward and epicardial contours 10% inward. For images with motion artifacts, they were reviewed for quality, and rescanning was conducted when necessary to obtain images of adequate quality. T1ρ values were measured for each slice and segment. Short-axis cine images were analyzed using CVI42 software (Version 5.6.6, Circle Cardiovascular Imaging Inc., Calgary, Canada). They provided left ventricular ejection fraction (LVEF), cardiac index (CI), end-diastolic volume index (EDVi), end-systolic volume index (ESVi), stroke volume index (SVi), and mass index (Mi). Two observers (C.H. and H.X. both with 2 years’ experience in cardiac MRI) independently performed all analyses, blinded to each other’s results. A senior observer (X.L. with 15 years’ experience in cardiac MRI) adjudicated when there were discrepancies.
Inter-and intraobserver reproducibility
Intra- and inter-observer reproducibility of T1ρ mapping was evaluated in a random subset of 20 participants. One observer (C.H.) performed T1ρ analysis for each left ventricular segment twice, with a minimum interval of 2 weeks between measurements. A second blinded observer (H.X.) independently analyzed the same cases to assess interobserver reproducibility.
Statistical analyses
Statistical analysis was performed in SPSS 26.0 (IBM Corp, Armonk, NY), a post hoc power analysis was conducted using G*Power software (version 3.1.9.7). A p value < 0.05 was considered statistically significant. Data were assessed for normality using the Shapiro-Wilk test. Continuous normal variables were expressed as mean ± standard deviation (SD). Student’s t-test analyzed the differences in T1ρ values between males and females at each spin-lock frequency. One-way ANOVA evaluated differences in T1ρ values across spin-lock frequencies, with post-hoc pairwise comparisons using LSD tests with Bonferroni adjustment. Intra- and inter-observer reproducibility were assessed by intraclass correlation coefficients (ICCs) analysis. Scan-rescan reproducibility was evaluated by coefficient of variation (COV) and ICC.




留言 (0)