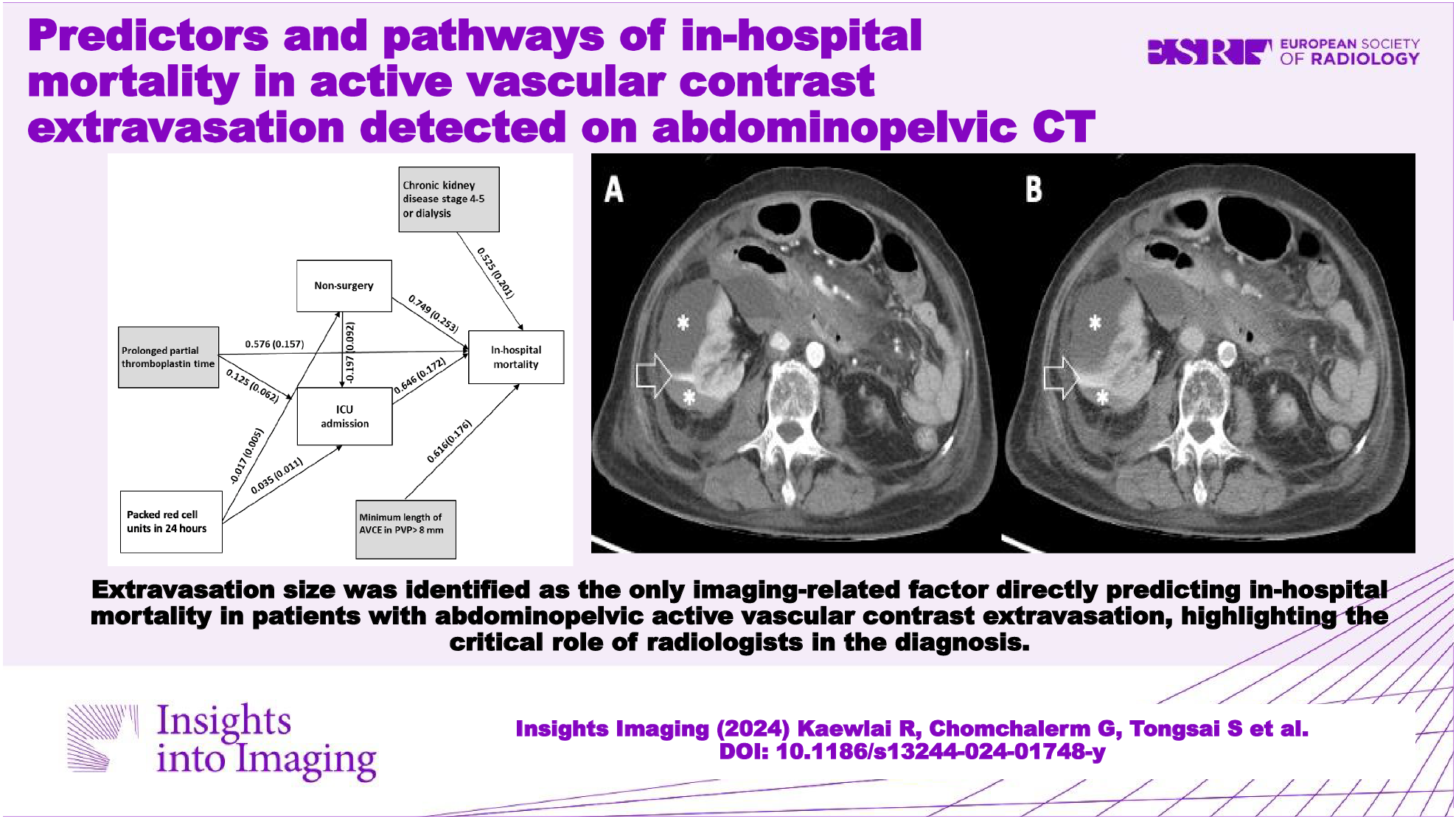
Our investigation identified factors associated with mortality in patients with abdominopelvic AVCE. Using path analysis, we further explored the complex interrelations among these factors and their effects on in-hospital mortality. The analysis modeled direct and indirect relationships within variables. After model specification, simplification, and evaluation of fit indices, the final model was chosen for its robustness in capturing the relationships among the variables, providing a comprehensive representation of the underlying mechanisms contributing to in-hospital mortality. We identified AVCE size as the only imaging parameter directly impacting mortality, highlighting the critical role of radiologists in not only detecting but also carefully evaluating AVCE features along with the clinical context. Factors such as age, coagulopathy, and vital signs are important considerations for further treatment. Additionally, non-imaging factors such as CKD4-5 or dialysis and prolonged PTT directly impacted mortality, with the latter also indirectly influencing mortality via ICU admission. PRC transfusion affected mortality through nonsurgery and ICU admission. These findings enhance our understanding of complex bleeding-related deaths, which occur through various factors and stages due to complications stemming from the initial blood loss. Some of these factors may be modifiable, offering potential value in clinical practice.
In-hospital mortality of patients with AVCE
Mortality rates of abdominopelvic AVCE vary according to sites of origin, causes, and underlying conditions. These have been reported to be between 15 and 75% in nontraumatic [8,9,10] and 18% and 32% in traumatic conditions [6, 11,12,13]. Our investigation concurred with other reports and showed similar rates of in-hospital mortality in patients with AVCE, which are particularly high for free-space AVCE than the rest.
Factors associated with in-hospital mortality
Three independent predictive factors (CKD4-5 or dialysis, prolonged PTT, minimum AVCE length) directly influenced in-hospital mortality in our investigation but one (PRC transfusion) acted through mediators. These mediators were nonsurgery and ICU admission.
CKD4-5 or dialysis
Our study emphasizes that severe CKD or dialysis independently predicted in-hospital mortality in AVCE patients. Severe CKD can instigate abdominopelvic bleeding, especially within the GI tract [14, 15], and even among those undergoing percutaneous coronary intervention bleeding [16]. Uremic bleeding, observed prior to dialysis, stems from primary hemostasis defects like platelet dysfunction and anemia [17]. Even dialysis patients face persistent bleeding risks due to continuous platelet activation during hemodialysis [18]. Recognizing these underlying conditions is crucial as they can worsen the morbidity and mortality of patients with active bleeding.
Prolonged PTT
We found that prolonged PTT, a measure of the intrinsic clotting pathway, played a crucial role in active bleeding scenarios. Prolonged PTT may signify underlying coagulation abnormalities such as liver disease and disseminated intravascular coagulation. Conversely, in cases of ongoing bleeding, prolonged PTT indicates consumptive coagulopathy, where clotting and breakdown occur simultaneously [19]. Previous studies have consistently associated prolonged PTT with heightened morbidity and mortality in bleeding conditions. For instance, in postpartum hemorrhage, individuals with prolonged PTT and low fibrinogen levels were more likely to require surgical intervention and experienced severe outcomes [20]. Similarly, patients receiving heparin with PTT markedly above the therapeutic range faced an increased risk of early mortality [21]. Given the multifaceted nature of active bleeding, our findings underscore the critical role of PTT in predicting in-hospital death.
Larger size and progressive heterogeneity of AVCE
The urgency of intervening in AVCE based on CT findings is well-established due to its associated high mortality rates [6]. However, determining which specific characteristics render one AVCE more lethal than another has remained unclear. Our CT analysis identified the minimum AVCE length in the PVP CT as the sole predictor of in-hospital mortality, with a cutoff of 8 mm (AUC 0.589, p = 0.017). Additionally, AVCE heterogeneity (measured by SD values) and progression (percentage changes in SD values between CT phases) were correlated with mortality. Heterogeneity suggests a higher bleeding rate, becoming more varied as leaked contrast mingles with blood. While dual- or triple-phase CT scans are typically recommended for suspected nontraumatic hemorrhages [22, 23], our study supports their utility in evaluating patients with suspected AVCE regardless of traumatic or nontraumatic history [24, 25].
Treatment other than surgery
Advancements in bleeding control techniques, such as endoscopy and TAE, have reduced the reliance on surgical interventions for active abdominopelvic bleeding. Nontraumatic hemorrhages now favor endoscopic methods for upper and lower GI bleeding [26, 27], while TAE gains prominence for bleeding in solid abdominal organs, the retroperitoneum, and the abdominal wall [8, 10, 28, 29]. Despite these advancements, our study found that surgery yielded better outcomes in terms of in-hospital mortality. Among 43 patients who survived after surgery, 29 had trauma-related active bleeding, predominantly in intramuscular (n = 9), intraperitoneal (n = 8), and retroperitoneal/extraperitoneal spaces (n = 5 each). Surgery’s success may be attributed to specific demographics, with more traumatic cases among survivors, compared to non-survivors with nontraumatic bleeding. This highlights the ongoing significance of surgery in managing abdominopelvic trauma, with procedures like damage-control surgery and exploratory laparotomy playing vital roles [29]. However, potential selection biases may exclude surgically managed patients in poor health, redirecting them to alternative treatments due to perceived risks. This underscores the persistent relevance of surgery as a viable strategy for active bleeding in selected cases, complementing evolving nonsurgical approaches.
PRC transfusion
In our study, we found that PRC transfusion indirectly influenced mortality, with lower rates associated with decreased mortality in nonsurgery settings and higher rates linked to higher mortality in ICU settings. The complex interaction of PRC transfusion with other factors preceding deaths was illuminated through our analysis. In cases of hemorrhagic shock, the massive transfusion protocol necessitates large quantities of PRC and fresh frozen plasma in a large quantity [30, 31]. However, a restrictive strategy in maintaining lower hemoglobin levels is increasingly favored in ICU patients with anemia, sepsis, and GI hemorrhage, due to accumulating evidence suggesting mixed or non-beneficial outcomes with PRC transfusion [32, 33]. In trauma cases, the relationship between PRC transfusion and mortality seems to depend on the predicted risk of death, with transfusion associated with increased mortality in patients with a predicted risk below 20% [34]. Our study shed light on the indirect effects of PRC transfusion before death, offering valuable insights for future research.
This investigation has several limitations. First, it is a single-center retrospective study with a relatively small sample size, even though it met the precalculated sample size value. Second, not all instances of AVCE received angiographic, endoscopic or surgical confirmation, potentially affecting the study’s inclusiveness. However, CT reinterpretation by three radiologists served as a reference standard, adhering to established definitions. It is essential to acknowledge that AVCE is an ongoing process influenced by various factors like time, treatment, and underlying pathology, and any visualization method can only provide a single snapshot of the disease’s progression. Third, some factors contributing to mortality may not have been collected and thus were not studied. These may include other blood components such as fresh frozen plasma and pooled thrombocytes. Fourth, consolidating all instances of AVCE, regardless of their underlying causes, into a single category labeled “nontraumatic” might potentially limit the practical applicability of these factors. Nonetheless, this approach has enabled us to gain insights from a broader spectrum of patients with active abdominopelvic bleeding, which was not previously understood. Fifth, in-hospital mortality is significantly confounded by the treatment administered in each case, which can impact the mortality rate. It may not always be secondary to bleeding in the abdomen and pelvis, particularly in trauma patients. In some cases, complications of prolonged hospitalization may have led to death. To address these limitations more effectively, further investigation employing a case-control design or randomized control trial may be beneficial. Finally, we recognize that the near-perfect fit indices of our final path model might raise concerns about overfitting. However, we believe that the model was built on robust theoretical foundations and meticulously specified to distinguish substantive effects from random noise.
In conclusion, several clinical and CT factors had direct and indirect influence on in-hospital mortality in patients presenting with AVCE on abdominopelvic CT. Larger AVCE directly increased mortality, underscoring the crucial role of radiologists in detecting and characterizing these findings.




留言 (0)