Design
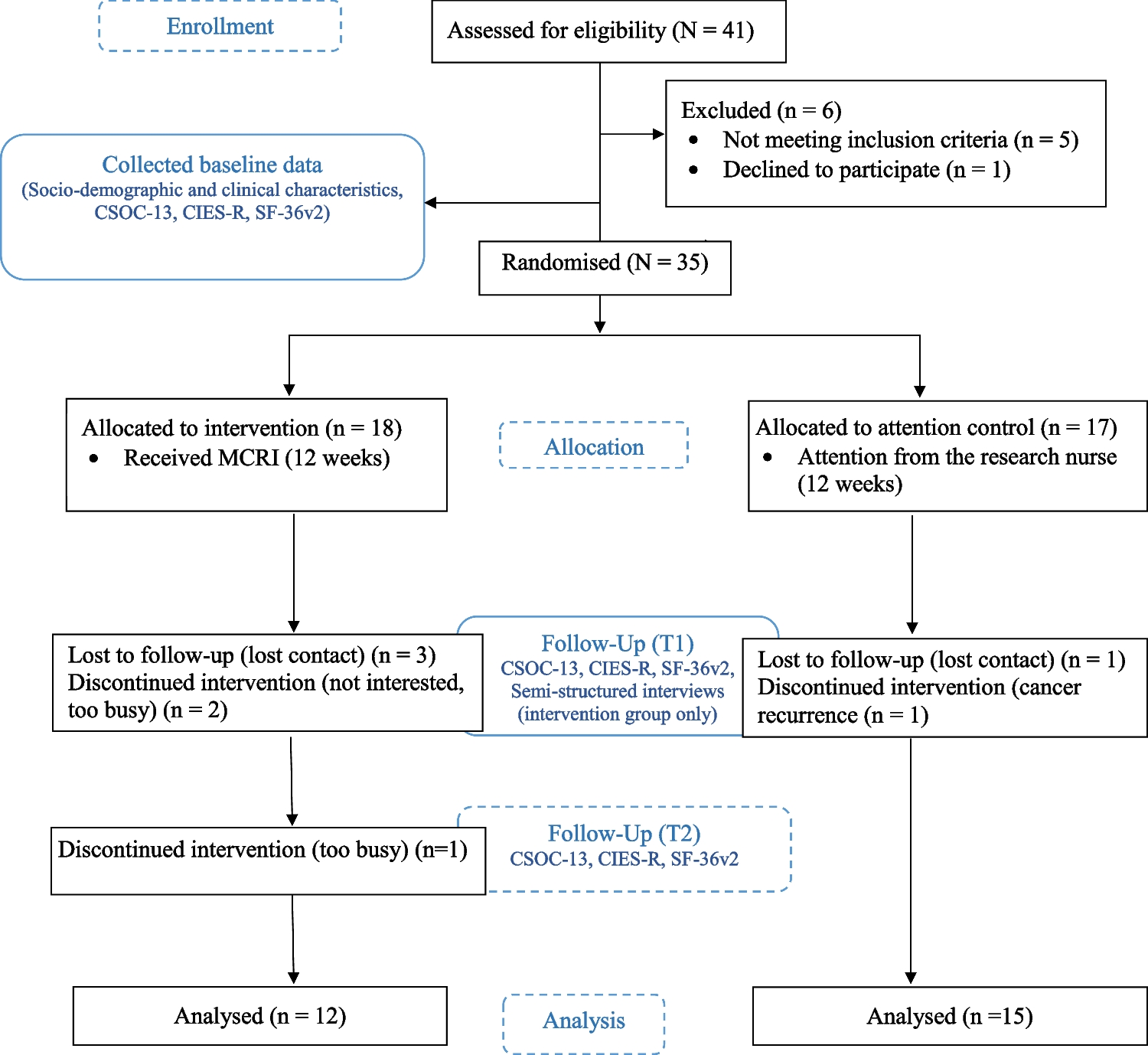
An assessor-blind, parallel pilot randomised controlled trial was conducted in the gynaecological or breast oncology clinics at two regional hospitals in Hong Kong. This study followed the CONSORT extension to pilot trials [25] and the CONSORT-EHEALTH checklist [26].
Participants
Inclusion criteria for recruitment included women with primary diagnosis of FRC; within 3 months of completion of intensive cancer treatments (e.g. surgery, radiotherapy, and/or chemotherapy) but can be on maintenance therapies such as tamoxifen, trastuzumab, and bisphosphonates; over 18 years old; able to understand spoken Cantonese and to read Chinese; having internet-connected computing devices or smartphones; and consenting to participate. Individuals who had health conditions that could potentially affect their ability to understand information and complete questionnaires, such as visual impairment or pre-existing psychosis based on medical records and verification during the recruitment process, were excluded from the study. Based on the rule of thumb proposed by Browne [27] that the sample size for a pilot study should be at least 30 and the previous pilot study on the similar patient sample population [14, 28, 29], we aimed to recruit 40 participants, with 20 diagnosed with breast cancer and 20 diagnosed with gynaecological cancers.
Randomisation, allocation concealment, and blinding
The enrolled participants were randomised in a 1:1 allocation ratio by an independent statistician using computer-generated random numbers. The sequentially numbered, opaque sealed envelopes were used to ensure allocation concealment. All data assessors, including those administering the instruments at follow-ups, were blinded. However, due to the nature of the intervention, it was not possible to blind the participants, the interviewer, and the nurse intervener.
The intervention
Participants in the intervention group received the 12-week MCRI delivered by a research nurse. The MCRI is largely based on the web-based version of WWACPHK [14]. In the current study, we have incorporated the key concepts of the Salutogentic Model [20] (providing generalised and specific resistance resources to enhance comprehensibility, manageability, and meaningfulness) into WWACPHK, developed an mobile application (app) with interactive features, and added a nurse counselling component. In brief, the MCRI featured WWACPHK app as a generalised resistance resource and three individual telephone counselling sessions provided by the nurse as a specific resistance resource to enhance women’s SOC after cancer treatment. The intervention participants were given access to the WWACPHK app, which included 30 modules covering topics such as healthy diet, exercise, menopause-related symptoms and management, sleep, sexuality, body image, pelvic floor exercises, stress management, chronic disease prevention, and cancer screening. New information was released to the app daily for the first 3 weeks and then weekly for the remaining 9 weeks. Participants could also communicate with the research nurse through instant messaging within the app. The research nurse monitored participants’ activity on the app and provided reminder telephone calls if their accounts remained inactive for a week or more. Moreover, the research nurse conducted telephone counselling sessions with the participants in weeks 1, 6, and 12 which aimed to empower participants by instructing them on how to use the app, providing tailored health information, encouraging them to reflect on their beliefs, assumptions, knowledge, and goals to promote comprehensibility, manageability, and meaningfulness.
Participants allocated to the attention control group received basic information about the follow-up schedule during the baseline data collection. To minimise the effect of attention, participants in the control group also received attention from the research nurse during the same time period as the intervention group through telephone calls at weeks 1, 6, and 12. The nurse delivered general greetings and did not provide any specific interventions. After the completion of the study, participants in the control group received the eBook version of WWACPHK.
MeasurementsFeasibility
The recruitment rate (number of participants recruited per month), consent rate (number of consented participants divided by the number of eligible participants), retention rate (number of participants included in final analysis divided by the number of consented participants), counselling session attendance rate, percentage of modules accessed, and number of days active were recorded to assess feasibility.
Intervention outcomes
The Chinese version of the Sense of Coherence 13-item Scale (CSOC-13) was used to assess SOC, with items clustered in meaningfulness, manageability, and comprehensibility domains. Higher scores indicate higher SOC, and the scale has shown validity and consistency among Chinese women with cervical cancer [30].
Cancer-specific distress was measured by the 22-item Chinese version of the Impact of Events-Revised Scale (CIES-R), with items clustered in intrusion, avoidance, and hyperarousal domains. Higher scores indicate greater distress, and the scale has demonstrated good internal consistency [31].
The Hong Kong Chinese version of the MOS 36-item Short Form Health Survey version-2.0 (SF-36v2) was used to measure HRQoL, with items clustered into eight domains, including physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. These eight domains can be further aggregated into physical health component and mental health component summary scores. Higher scores indicate better HRQoL, and the scale has shown good validity, consistency, and reliability among the adult population in Hong Kong [32].
Acceptability
To assess the participants’ acceptability of the programme, individual semi-structured interviews were conducted with participants in the intervention group via telephone calls to collect views and comments on the MCRI. All interviews were audio-recorded. A co-author conducted the interviews with reference to an interview guide (Supporting information S1).
Demographic and clinical characteristics
The demographic and clinical characteristics of the participants were collected using a data collection sheet which included age, education level, monthly household income, marital status, number of children, length of residence in Hong Kong, religious beliefs, type and stage of cancer, treatment modality for the disease, and time since treatment completion.
Data collection
The research nurse approached eligible patients in the gynaecological or breast oncology clinics and explained the aims of the study. Information sheets about the study and consent forms were provided. Upon obtaining written consent, the patient’s demographic data were collected, and the instruments were administered during face-to-face interviews at baseline (T0) before random allocation. The instruments CSOC-13, CIES-R, and Hong Kong Chinese SF-36v2 were reassessed on completion of the programme (T1) and 12 weeks after completion (T2) by a blinded research assistant. Following programme completion, intervention participants were invited to participate in recorded telephone interviews to share their experiences and thoughts about the programme. To minimise potential experimenter influence, a co-author with rich experience in conducting qualitative interviews with cancer patients facilitated the telephone interviews with reference to the interview guide. Each interview lasted from 14 to 45 min. All participants did not receive any financial compensation for participation in the study.
Data analysis
Statistical analyses were performed using SPSS version 28 (IBM Corp., Armonk, NY), and all tests were done using a two-sided 0.05 level of significance. Due to the challenge of assessing the normality of the continuous variables with the small sample size, non-parametric tests were adopted for all inferential analyses. Baseline characteristics between the intervention and control groups were compared using Mann–Whitney, chi-square, and Fisher’s exact test, as appropriate. The changes in outcomes at T1 and T2 with respect to T0 between the intervention and control groups were compared using the Mann–Whitney test and Cohen’s d effect size (95% confidence intervals). According to Cohen [33], effect sizes of 0.2 were considered small, 0.5 medium, and 0.8 large.
The interview recordings were transcribed verbatim, and the transcripts were analysed using NVivo 2020 (QSR International, USA). The thematic analysis approach by Braun and Clarke [34] was adopted to analyse the interview transcriptions. After reading one-third of the transcripts to become familiar with the data, two researchers (the first author and the interviewer, both involved in designing the study) independently identified initial codes from the early transcripts and then condensed similar codes into subthemes and themes through iterative discussions. This process involved continuous team comparisons and discussions to refine the subthemes and themes until reaching a consensus. Finally, the subthemes, themes, and selected quotations were translated by the interviewer fluent in both English and Chinese. The translations were then confirmed by the first author to ensure semantic equivalence.
Rigour
Lincoln and Guba [35] outlined the four criteria for developing trustworthiness in qualitative research, including credibility, transferability, dependability, and confirmability. Transferability concerns about the generalisability of the findings to other settings or groups, which was not the aim of the qualitative study [36, 37]. To improve credibility, we recruited an independent researcher to conduct the interviews, provided examples of representative quotations, depicted the role and experience of the researchers, and had two researchers independently performed analysis and sought agreement on the final themes, subthemes, and codes [36]. To enhance dependability, the same interview guide (Supporting information S1) was used to guide all interviews [36]. Finally, to maximise confirmability, we provided a rich presentation of the quotes from the interviews organised under respective codes, subthemes, and overarching themes (Supporting information S2) [37].

留言 (0)