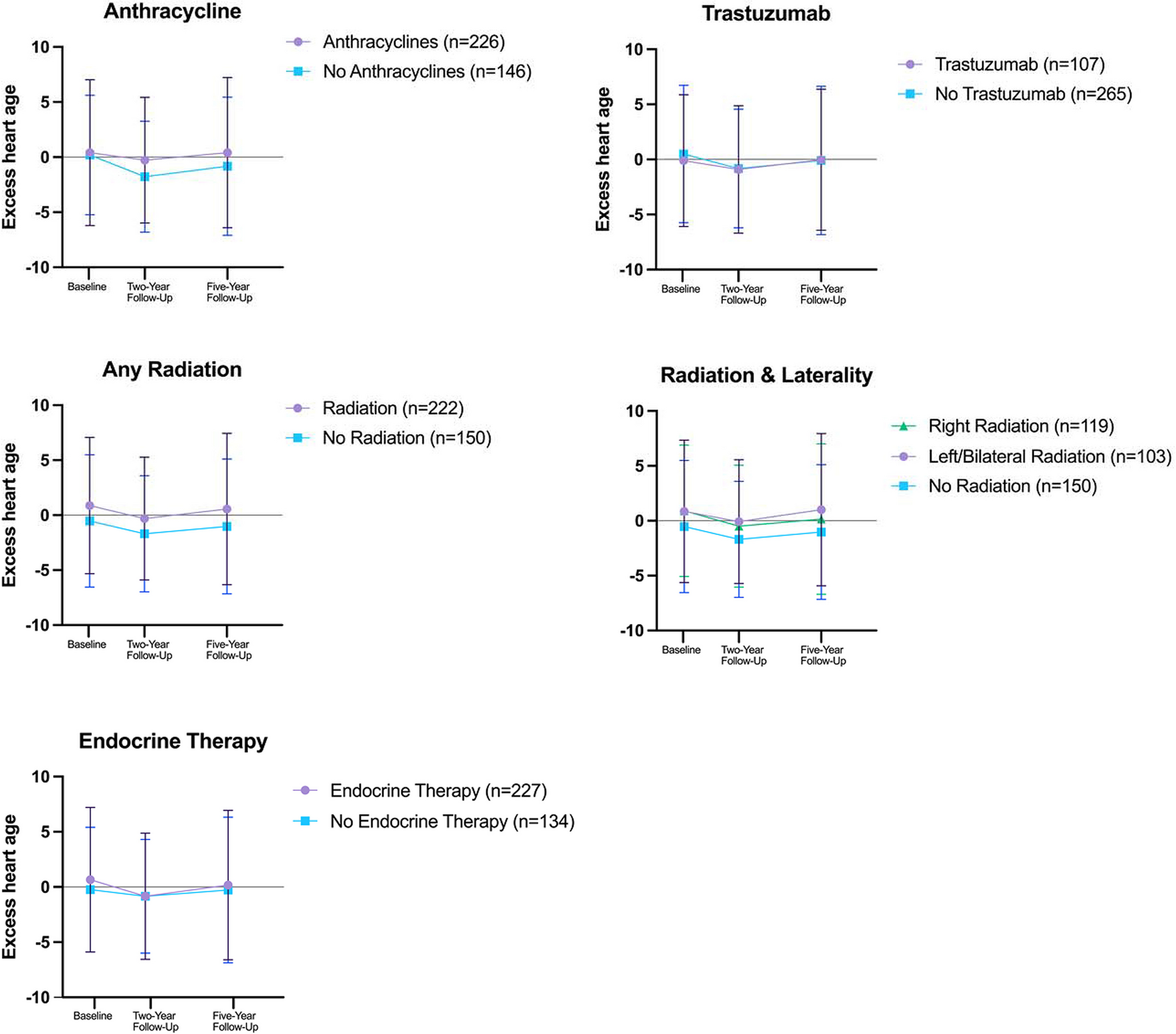
In this cohort of young breast cancer survivors, most women had minimal excess heart age at the time of breast cancer diagnosis, suggesting a cardiovascular disease risk comparable to the nationally reported average of excess heart age for women aged 30–39 years [20]. However, nearly 1/3 of young breast cancer survivors in this cohort experienced a change in their excess heart age from breast cancer diagnosis of ≥ 2 years after 5 years of follow-up. Among cancer treatments, radiation, especially left-sided radiation, was associated with higher cardiovascular disease risk after five-years of follow up, while other cancer treatments were not.
While studies have evaluated excess heart age in other patient populations[21,22,23,24,25], only one study has previously assessed excess heart age among breast cancer survivors. This prior study was conducted within an Alabama health system, and the mean excess heart age was 4.2 years at baseline for 152 women under 45 years [15]. The YWS cohort includes mostly non-Hispanic White patients largely based in Massachusetts, who have a statewide reported average excess heart age much lower than Alabama (3.5 vs 8.1 years, respectively) [20]. These differences are likely attributable to regional differences in cardiovascular disease risk factors including body mass index, comorbidities, and physical activity.
We have extended prior research by assessing the association between breast cancer treatment and excess heart age among young five-year survivors in a relatively large prospective cohort (twice the sample size of the Alabama study). We observed higher cardiovascular disease risk at five years for women treated with radiotherapy after breast cancer diagnosis. Cardiovascular disease, especially ischemic heart disease, is a long-term effect of radiation therapy with disease incidence occurring 10 + years after initial treatment [5, 26], with prior studies demonstrating increased risk after left- compared to right-sided radiotherapy [5, 19]. Since none of the patients in our study experienced cardiovascular events at 5 years follow-up, excess heart age may be capturing changes in cardiovascular risk factors, such as increasing blood pressure or body mass index, that may place young female survivors at risk for developing premature radiation-related cardiovascular disease, especially given the accentuated risk due to younger age at radiation exposure [13, 19, 27]. Further, the increased prevalent excess heart age observed after right-sided radiotherapy in one of our models may be related to an indirect effect with obesity, as women who are more obese and have large breasts may be less likely to receive mastectomies due to cosmetic challenges with surgical reconstruction and may be more likely to have partial mastectomy with radiation [28]. These higher-risk women may also have other co-occurring diseases or pre-existing risk factors that could potentially increase their risk of developing cardiovascular disease. Importantly, modern radiation treatment practices for cardioprotection, including positioning to protect the heart such as breath-hold or prone positioning, increased precision using image guidance, and proton therapy as an alternative energy source, could potentially improve long-term radiation-related cardiovascular disease risk [29]; however, we did not have these data available.
In the present analysis, we did not observe associations between excess heart age and anthracyclines, trastuzumab, or endocrine therapy that were found in a prior study [15]. This was reassuring and may be related to increased awareness about potential adverse effects of chemotherapy and resultant healthy lifestyle changes through cancer treatment and survivorship that mitigate cardiovascular disease risk [30]. It is also possible that compared to older patients, young women treated with anthracyclines and trastuzumab may be more resilient against cardiotoxic damage due to the relative lack of baseline cardiovascular disease risk factors [3, 4, 31]. However, it is important to note that subclinical changes in cardiac function that may occur after anthracyclines or trastuzumab receipt, especially when used together, could not be assessed with this excess heart age tool, and risk of cardiovascular disease among young breast cancer survivors may be heightened long after the five years of follow-up in this study as seen in AYA cancer survivors 10 + years after diagnosis [10].
Although we did not observe significant associations between anthracyclines or trastuzumab and excess heart age, clinical guidelines have stressed the importance of monitoring for and preventing cardiomyopathy in patients treated with anthracyclines or trastuzumab since early detection can lead to improved outcomes. Current clinical guidelines for breast cancer survivors do not emphasize screening after radiotherapy [12, 13]; however, we observed significant associations between radiation and subsequent elevated excess heart age. Thus, the clinical implications of this study include cardiovascular surveillance after radiotherapy and management of modifiable lifestyle factors (e.g., physical activity, weight management, hypertension control) to improve cardiovascular disease risk after radiation treatment. Excess heart age could be used in survivorship care to improve provider-patient communication regarding cardiovascular disease risk [18] and could facilitate healthy lifestyle changes or referral for additional screening as well as early detection and intervention for subclinical cardiovascular disease in high-risk women.
Findings of this research should be interpreted in the context of certain limitations, including our inability to assess cardiovascular risk associated with specific chemotherapy regimens (i.e., joint effects of anthracyclines with trastuzumab), radiation dose, or endocrine therapy type (tamoxifen versus aromatase inhibitors) due to inadequate statistical power. Further, five years of follow-up may not be a sufficient length of follow-up for young breast cancer survivors who are relatively healthy at diagnosis and due to the long latency of treatment-related cardiovascular disease, warranting future extended assessments of cardiovascular disease risk (e.g., 10 or more years after breast cancer diagnosis). The tool excess heart age may not fully capture the full range of cardiovascular risk prior to cancer treatment receipt, and we were also unable to assess left ventricular function which may have characterized subclinical changes from diagnosis to after treatment. Finally, the use of heart age is not validated in cancer populations, and studies are needed to inform cardiovascular disease risk associated with potentially cardiotoxic treatments, especially in patients where traditional cardiovascular risk estimation tools are unavailable. Future research should consider the cardiotoxic impact of newer regimens such as immunotherapies and cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors and the potential effects of ovarian suppression on cardiovascular disease risk.
Nevertheless, our finding of potentially increased risk of cardiovascular disease for a substantially small group of young breast cancer survivors, especially after left-sided radiotherapy, warrants future investigation especially given the long survivorship and long latency of cardiovascular disease. Cardiovascular disease risk tools that incorporate cancer treatment predictors into models are needed to appropriately identify high-risk patients, especially among young survivors who have a low absolute, but higher relative risk than age-matched non-cancer controls. Extended follow-up of the YWS cohort as well as evaluation of this risk in other cohorts may further quantify cardiovascular disease risk and long-term cardiac outcomes in young breast cancer survivors.

留言 (0)