
記住我
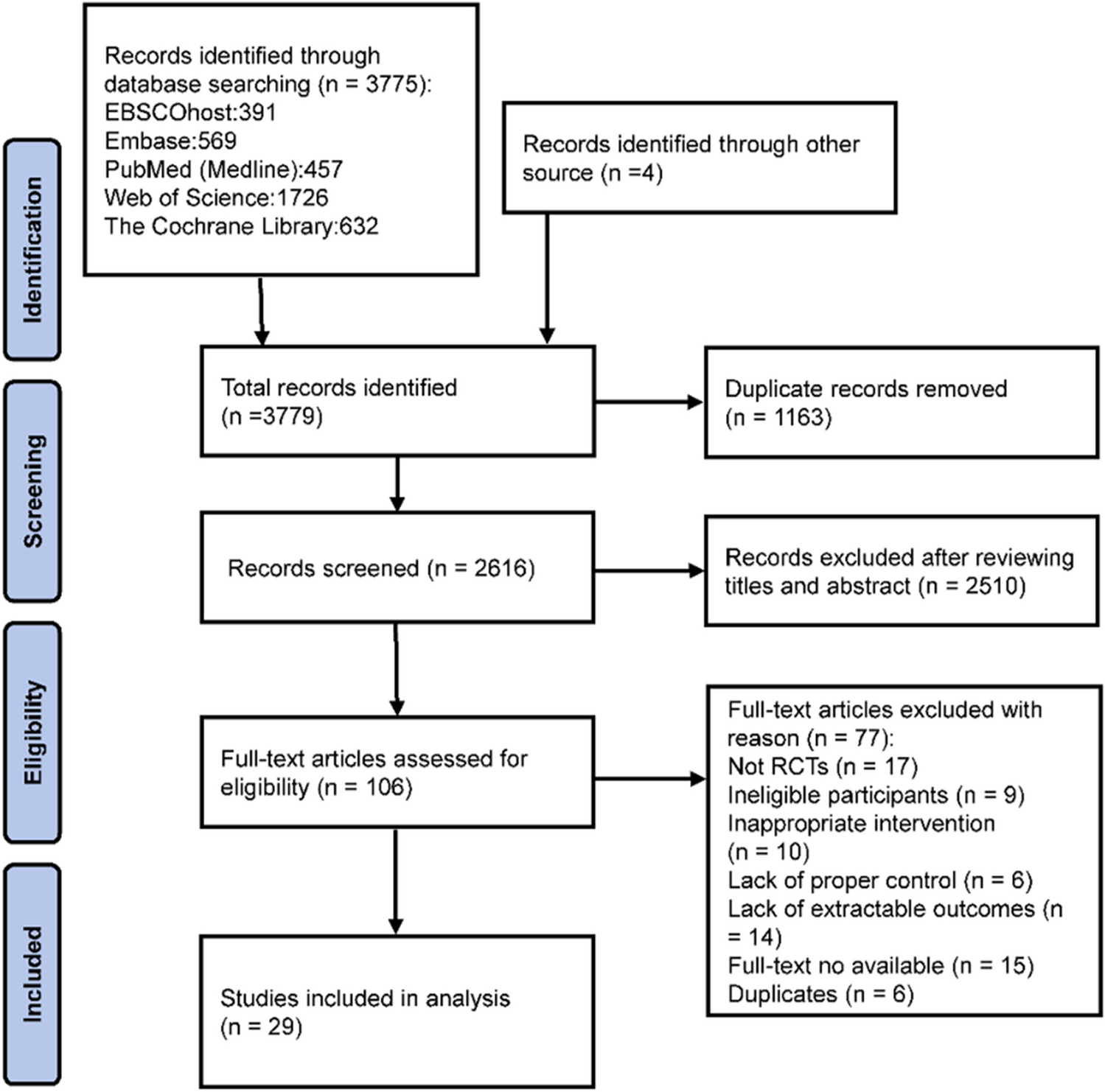
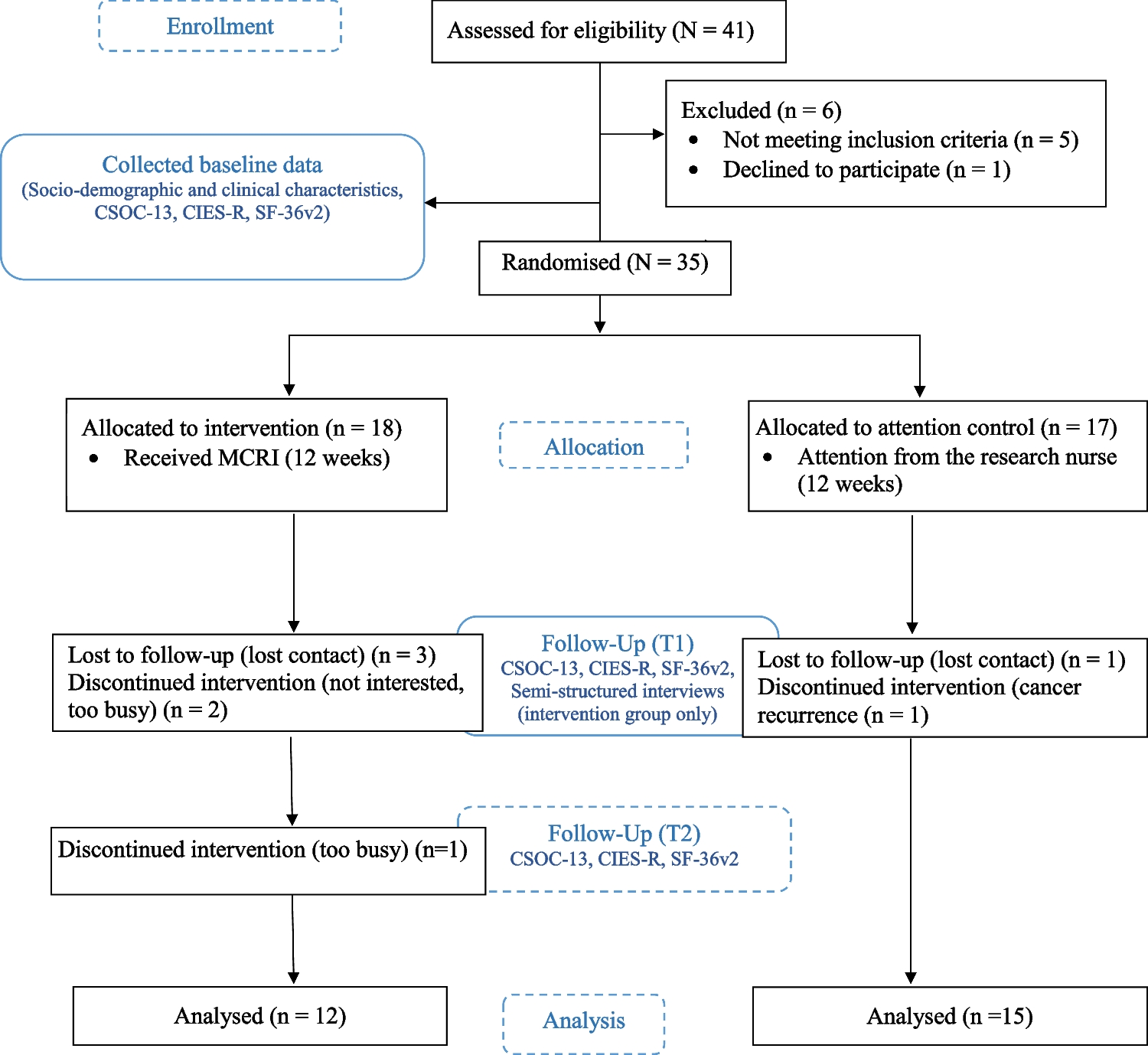
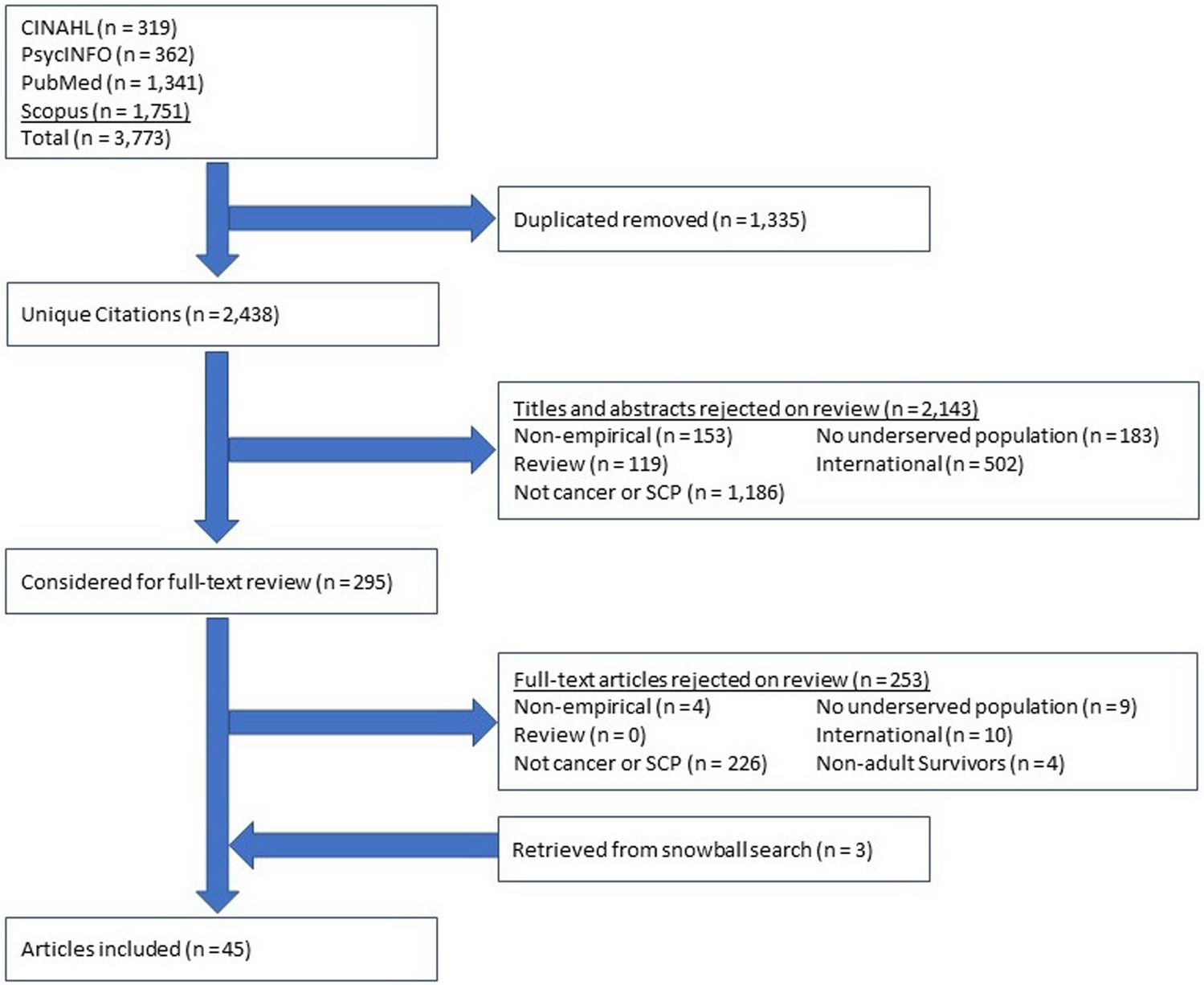
Our keyword search identified an initial yield of 2438 unique articles. Studies in step 1 were most frequently excluded for not having a focus on cancer or SCPs, being conducted outside of the USA, and not targeting a group that is underserved (see Fig. 1). After excluding these citations, 295 articles were included in step 2. The primary reasons for exclusion at this stage included not having a focus on cancer or SCPs and being conducted outside of the USA. After applying all the exclusion criteria in the review of full-text articles, 42 studies were included. The snowball search yielded an additional 3 articles. Data was extracted from the final set of articles. A total of 45 studies were included in this systematic review published between 2009 and 2023 (see Appendix 2 for a list of included studies).
Fig. 1 Study characteristics
Study characteristicsTwenty-three of the included studies used quantitative methods, 14 used qualitative methods, and 8 used mixed methods. Most quantitative studies (16/23) were cross-sectional studies, 2 were cohort studies, 4 were randomized control trials (RCTs), and 1 was a single-arm study. Six of the 14 qualitative studies used focus group discussions, 4 used semi-structured interviews, 3 used community-based participatory research (CBPR) approaches (consensus meetings, focus groups, interviews), and 1 was a think aloud. Studies varied with respect to the population targeted, type of SCPs administered (treatment summary or follow-up care plan), and the cancer type of interest. The majority of studies focused on Black populations followed by studies targeting diverse populations of more than one group that is underserved. In addition, most studies focused on breast cancer (n = 29) survivors, followed by colorectal (n = 11), gynecologic (n = 11), and prostate cancer (n = 10) survivors.
Theme 1: Benefits of survivorship care plansOne recurring theme we identified was related to benefits from SCPs in 18 articles (see Table 1). Eleven studies were quantitative composed of 3 RCTs, 1 single-arm trial, 6 cross-sectional studies, and 1 cohort study. Four were qualitative composed of 2 CBPR (focus groups, RAND-Delphi method, and interviews), 1 focus group study, and 1 think aloud. Two of the 3 mixed methods studies were single-arm studies, 1 was an RCT, and all 3 used semi-structured interviews. Participants including both healthcare providers and survivors across different studies found the SCP to be useful [25, 26]. Some articles studied the effects of SCP interventions that entailed some form of patient navigation through counseling with nurses or nutritionists [27,28,29]. For example, Maly and colleagues conducted an RCT of SCPs for a low-income, predominantly Latina population of breast cancer survivors [29]. This study examined the effects of treatment summaries and SCPs coupled with a nurse counseling session on physician implementation of survivorship care. Participants in the intervention group reported greater physician implementation of survivorship care such as treatment of hot flashes. Herschman and colleagues conducted an RCT among women with early-stage breast cancer [28]. Participants in the intervention group met with a nurse/nutritionist who provided them with a treatment summary, surveillance, and lifestyle recommendations. This study found no significant improvements in patient-reported outcomes like treatment satisfaction, survivor concerns, depression, and impact of cancer; however, the intervention was associated with decreased worry in the short term. In a separate publication, this group also found that the intervention was effective at changing behaviors and improving knowledge in the short term and was less effective among Hispanic people in improving attitudes towards healthy eating and physical activity when compared with non-Hispanic White individuals [27].
Table 1 Benefits from survivorship care plans among underserved populations (n = 18)In place of clinic-based interventions, Casillas and colleagues developed and tested a culturally tailored intervention that included family members of Latino adolescent and young adult survivors and a community health advocate. This intervention resulted in increased knowledge and confidence in the management of survivorship care for both survivors and family members [30]. In another study, Nápoles and colleagues combined a culturally tailored paper SCP, Spanish language mobile health (mHealth) app, and telephone coaching to address survivorship care in Spanish-speaking Latina breast cancer survivors [31]. This intervention reduced fatigue and distress among survivors, increased knowledge of care resources, increased physical activity, improved general well-being, and provided a sense of accountability and motivation through feedback from the telephone coaching and mHealth app [31]. Baseman and colleagues explored the acceptability and feasibility of an SCP in the form of an mHealth app for rural survivors [32]. Both survivors and their providers noted greater self-efficacy and communication on account of the journaling and reports features. Participants in this study also reported that the reminders feature was useful for surveillance [32].
In a survey study of rural cancer survivors, Lewis-Thames and colleagues found that rural survivors receiving written post-treatment survivorship communication had greater odds of reporting timely follow-up care [33]. In an evaluation of a structured care plan called Care Sequence in five safety-net institutions and five non-safety-net institutions, the SCP was perceived as useful [26]. Patient self-management metrics like clarity on the timing and sequence of care, as well as care delivery metrics like flu vaccinations, were higher in those who received Care Sequence. These benefits were similar for both safety-net and non-safety-net survivors. Survivors also cited benefits like having structure to stay focused on the task, and ability to see a timeline, and proactively seeking answers [26]. Similar benefits were mentioned by healthcare providers and survivors in the qualitative study by Ko and colleagues which found the SCPs helped patients become proactive about their care and formulate questions for their healthcare visits [34].
Theme 2: Receipt of survivorship care plansSixteen studies brought attention to cancer survivors and their likelihood of receiving an SCP (see Table 2). A majority of these studies were quantitative using cross-sectional designs (n = 13) with two studies using qualitative methods in the form of focus groups (n = 1) and semi-structured interviews (n = 1). Lastly, one study used both a cross-sectional design as well as semi-structured interviews (n = 1). Using a sample of cancer survivors from the LIVESTRONG Survivorship Center of Excellence Network sites, Casillas and colleagues used survey data and found that minority cancer survivors were significantly less likely to have an SCP [35]. In addition, minority cancer survivors had higher odds of reporting low confidence in managing their cancer survivorship care [35].
Table 2 Receipt of survivorship care plans among underserved populations (n = 16)Several cross-sectional studies using Behavioral Risk Factor Surveillance System (BRFSS) data also showed that cancer survivors with lower education [36,37,38,39] and income [36,37,38,39] and being uninsured [39] were less likely to report receiving SCPs. For example, Jabson and colleagues found that demographic characteristics were associated with the receipt of treatment summaries and follow-up care instructions [37]. More specifically, cancer survivors who reported completing less than a high school education and who reported household incomes lower than $50,000 had lower odds of reporting receipt of treatment summaries. Incidentally, this study also found that Hispanic cancer survivors were more likely to receive treatment summaries [37]. Wu and colleagues used BRFSS data and found that low-income breast cancer patients had lower odds of receiving follow-up care instructions from their providers [40].
Sabatino and colleagues examined the receipt of treatment summaries and follow-up instructions among African-American and Hispanic cancer survivors [41]. This study found that many recently diagnosed cancer survivors did not report receiving treatment summaries and written follow-up instructions. In addition, race and ethnicity were associated with lower reporting of summaries. DeGuzman and colleagues explored the needs of a sample of seven rural, low-income breast cancer survivors and their post-treatment survivorship care planning [18]. This study found that rural survivors had a lack of knowledge of post-treatment care, such as how to assess cancer recurrence. In addition, none of the women reported receiving or hearing about an SCP. While some women reported receiving a packet of information, there was no specific information provided.
Tawfik and colleagues implemented and evaluated a process of generating and delivering SCPs to patients and providers in a comprehensive cancer center that serves poor, rural, and minority cancer patients [42]. They reported that of all the SCPs ordered, about 85% were generated, and of those generated about a third (34.2%) were given to patients. Approximately half (48.9%) of SCPs were sent to primary care providers (PCP) by mail or fax, and 8.3% of these were received [42].
Theme 3: Needs and preferences of survivorsA third major theme was related to identifying the unmet needs and preferences of groups that are underserved with respect to the contents of SCPs. We identified 18 studies targeting Black, Latina, rural, and low-income cancer survivors (see Table 3). These studies were predominantly qualitative (n = 12) followed by 5 mixed-methods studies and 1 quantitative study. Most studies used focus groups (n = 5) or semi-structured interviews (n = 3). Others included CBPR (consensus meetings, focus groups, interviews, RAND-Delphi methods) (n = 3) and a think aloud study (n = 1). The mixed method studies were cross-sectional (n = 3) or single-arm trials (n = 2), and most used semi-structured interviews as well (n = 4).
Table 3 Needs and preferences of survivorship care plans (n = 18)ContentIn a qualitative study seeking to understand if SCPs are responsive to the needs of Black breast cancer survivors, Ashing-Giwa and colleagues found that while Black cancer survivors felt they would benefit from a well-organized SCP, they found several limitations to the SCP including inadequate information related to health history, the number and severity of comorbidities, health promotion, referrals to other specialists, and functioning [43]. Similar findings were presented in other qualitative studies [44, 45]. Burke and colleagues found that racial and ethnic minority women suggested that the SCP should include referrals to PCPs who were knowledgeable about their cancer and associated side effects. Women in this study also hoped the SCP would provide them with questions to ask their PCP [45].
The preferences for content differed based on the survivor or provider perspective. For example, minority cancer survivors noted wanting more information on lifestyle management, like physical activity and nutrition [43,44,45,46], whereas providers noted this type of content was less useful [47]. However, both groups agreed that information on genetic testing was an important addition [43, 45, 47]. Other needs expressed by Black survivors included referrals to spiritual care and culturally competent providers [43].
Tisnado and colleagues found numerous gaps and unmet needs among a sample of Latina breast cancer survivors [48]. While few women in this sample reported receiving an SCP, those who did receive an SCP were treated at a high-resource cancer center. In addition, participants also reported unmet needs in their survivorship care related to finances, continuity of care, and a lack of information related to symptom management.
Studies also assessed perspectives on the different components of SCPs. Preferred SCP elements included graphical representation of timing and sequence of care [26] and visual and auditory feedback from SCPs embedded in apps [31].
FormatIn terms of format, survivors differed in their preference for paper versus electronic SCPs. Hispanic breast cancer survivors preferred a print SCP [34, 46]. Conversely, rural participants in the study by Baseman and colleagues, which examined the feasibility and acceptability of SCP as an mHealth app, reported they did not want print SCPs [32]. In addition, rural PCPs preferred an electronic SCP that could be pushed from the oncologists’ electronic health record (EHR) to theirs [47].
Other format suggestions included the use of images [32, 46], improved readability [32, 44, 46], and tailoring for cultural appropriateness [43, 46]. Several preferences for layout were articulated across these studies: having key information on one sheet [26] and providing space for Black survivors to make notes [43].
Facilitating conditionsIn addition to content, format, and layout, survivors mentioned other factors that would facilitate the use of SCPs.
SCP aidsFor example, Hispanic survivors identified SCP aids in the form of patient navigators or coaches [31, 49]. Black survivors believed the information shared within SCPs should be discussed with their healthcare providers [44]. Studies also found that Hispanic patients also preferred aids like animated videos [34] or photonovelas [30] to provide SCP information.
Findings based on survivor perspectives suggest that discussing SCPs with the provider, and the timing when this discussion occurs, may be associated with the implementation of SCPs. Burke and colleagues reported that in-person review of SCPs, and delivery of SCPs at transition points in the cancer journey such as during active treatment, between active treatment and survivorship may facilitate the use of SCPs [45]. However, DeGuzman and colleagues reported that discussing SCPs in the final treatment appointment hindered knowledge retention by survivors [18].
LanguageIn a project aiming to translate and tailor the ASCO breast cancer treatment summary template to Latino breast cancer patients, the translated version was found to be more favorable than the ASCO template with respect to content, clarity, utility, cultural and linguistic responsiveness, and socioecological responsiveness [46]. Participants also liked that the template was bilingual, providing English text with Spanish translations adjacent to each other.
CoordinationBoth survivors and providers noted that the transition from cancer care to primary care was poor [47]. Survivors suggested that SCPs include referrals to PCPs knowledgeable about cancer side effects [45].
Theme 4: Barriers and facilitators to implementation of survivorship care plansLastly, we identified 19 studies related to barriers and facilitators of implementing SCPs predominantly based on healthcare provider perceptions (see Table 4). Seven of these studies were qualitative, 4 were quantitative, and 8 used mixed methods. The qualitative studies used semi-structured interviews (n = 3), focus groups (n = 2), CBPR (consensus meetings) (n = 1), and think aloud approaches (n = 1). Half of the quantitative studies were cross-sectional (n = 2), and the rest were a cohort study (n = 1) and an RCT (n = 1). Of the 8 studies using mixed methods, 3 were cross-sectional, 1 was an RCT, 3 were single-arm studies, and 1 carried out a suitability of materials assessment. The qualitative components included semi-structured interviews (n = 5), focus groups (n = 1,) and CBPR (consensus meetings) (n = 1). This theme is further divided into 4 categories.
Table 4 Barriers and facilitators of survivorship care plans in the healthcare setting (n = 19)Design-related factorsLyson and colleagues found that none of the SCPs from 53 health systems caring for vulnerable populations was concordant with IOM recommendations for SCPs [50]. In addition, designing SCPs with input from diverse populations and tailoring SCPs for readability and cultural appropriateness could facilitate the implementation of SCPs [32, 45, 50]. However, cost in terms of staff time and resources posed a barrier to developing understandable and comprehensive SCPs [50, 51].
In 2 of the 19 studies, SCPs were re-engineered with input from healthcare providers caring for groups that were underserved. Among providers in a rural research network, design features that facilitated the use of SCPs included modifications like the addition of a date field to determine the outdatedness of contents, clearly labeling the cancer diagnosis as early as possible, focusing on follow-up care rather than treatment summaries, and removing screening recommendations that were not cancer-related [47]. Further, providers indicated a preference for having a single SCP for patients and themselves. In a study among providers, participants found SCPs to be too long [52]. Yet, they did not recommend the removal of any sections; instead, they recommended bulleted lists or summaries at the beginning of the SCP and suggested having separate SCPs for patients and providers [52].
Provider preferences for layout were predominantly based on a study of PCPs, who suggested labeling the sections on an electronic SCP, the addition of a date-created field for easier navigation, labeling cancer diagnosis clearly, direct links from treatment information to supporting documents [47], and a reminder function for appointments [32].
Organizational factorsHealthcare providers noted the lack of coordination between primary care and oncology as a barrier to the use of SCPs [25, 42, 53]. Primary care providers in a rural primary care practice reported either rarely or never receiving SCPs from oncology providers, did not have a formal process to identify cancer survivors, and were unaware of how to access resources for cancer survivors [53]. In a study based in a comprehensive cancer center treating poor, rural, and minority survivors, PCPs reported a low receipt of SCPs from oncologists sent via mail or fax [42]. Suggestions to facilitate the use of SCPs included one to two pages of specific recommendations from oncologists [53], periodic updates by oncologists [25], and health systems using a standard SCP to share with PCPs [51]. Isaacson and colleagues noted an organizational barrier in assessing the use of SCPs for survivors treated by providers, whose only affiliation with health systems may be for the purpose of using surgical facilities [51].
Technology-supported SCPsTwo studies focused on mHealth approaches to implementing SCPs. Based on an RCT of an SCP embedded in an mHealth app among racial and ethnic minorities, Psihogios and colleagues found that trivia questions and health goal messages increased engagement with the app, and this engagement varied by the season when messages were sent [54]. Baseman and colleagues explored the feasibility and acceptability of a mobile breast cancer survivorship care app among six rural breast cancer survivors, four PCPs, and one oncologist [32]. Survivors in this sample were enthusiastic about having one location for all information such as contact information, their treatment records, insurance numbers, and other relevant information. All survivors perceived their existing ways of self-management, surveillance, and monitoring as inadequate. The tool was seen as a better way to self-manage their survivorship and track symptoms, wellness activities, and mood. Portability was also seen as a plus as they always had their mobile phones available. Providers identified interoperability with other healthcare systems as a potential barrier, expressing concerns about data quality if the system relied on manual data e
留言 (0)