This study highlights the importance of considering the specific type of health condition when explaining psychosocial functioning in CCS. Specifically, we found that CCS with secondary malignant neoplasms, gastro-intestinal conditions, endocrine, nervous systems, eye, or ear conditions reported worse psychosocial functioning. Most impact of health conditions was seen on the social and physical domain.
Almost half of CCS experienced at least one health condition. A recent study in the DCCSS-LATER 1 cohort showed that CCS experienced 2.8 times more health conditions than siblings [5]. In this study we found only a small impact of the overall presence and number of health conditions on psychosocial outcomes. Other studies found an association between health conditions and worse psychosocial outcomes among CCS [12,13,14], but health conditions are operationalized and analyzed in various ways across studies which hinders a direct comparison of results. The fact that overall presence and number of health conditions only explained a small percentage of the variation in psychosocial functioning in CCS suggests that other factors play a more important role in explaining psychosocial functioning, such as how CCS cope with the cancer experience and its late effects [26,27,28], associated subjective appraisals [29, 30], and CCS’ received social support [31,32,33]. In future research, a biopsychosocial approach could be utilized [34], taking into consideration a range of physical, psychological and social factors when explaining psychosocial functioning in CCS.
The specific types of health conditions had a larger impact on psychosocial outcomes than the presence and number of any health condition. This indicates that the specific types of health conditions play a more prominent role in explaining psychosocial functioning in CCS. Psychosocial interventions tailored to different types of health conditions may be necessary to improve outcomes. Out of the specific types of health conditions, having had a second malignant neoplasm was associated with most psychosocial outcomes (6). We found that CCS with secondary malignant neoplasms experienced worse psychosocial outcomes, such as increased anxiety and depression, with a moderate effect size. These outcomes may be attributed to uncertainty regarding the prognosis or to the fear of recurrence (FCR) which has shown to be associated to anxiety and depression [35]. The results of a systematic review indicated that FCR is relatively stable over time and that interventions are therefore of importance [36]. CCS who have experienced a second neoplasm may benefit from (contemporary) cognitive behavioral therapies focusing on processes of cognition such as worry, rumination [37], and the disappointment arising from having to face cancer once again.
Furthermore, we found that having an ear condition, defined as deafness or hearing loss, had a large negative impact on social functioning, and a moderate to large impact on higher depression. It is important to realize that only severe hearing problems are taken into account and other ear conditions, such tinnitus, are not included. The results are in line with research in the general population showing that hearing problems are associated with more depression and loneliness in adults [38]. Since hearing problems are not exclusive to CCS, unlike FCR, CCS might benefit from interventions [39] available in the general population to address hearing problems.
Out of the psychosocial outcomes, the most impact of specific types of health conditions was observed on general health perceptions. Eight types of health conditions showed a moderate to large association with general health perceptions. Therefore, CCS’ perception of diminished health seems to reflect their actual health status.
Given the substantial percentage of CCS experiencing clinically relevant health conditions, and the potential impact of some of these health conditions on psychosocial functioning, international guidelines recommend CCS to attend lifelong follow-up care [40], which can play an important role in monitoring and addressing late effects of childhood cancer. Most late effects may not be preventable or reversible. CCS can therefore benefit from learning coping strategies in psychological interventions to manage physical and psychosocial consequences of the cancer trajectory, as early as possible [27]. Also, many CCS desire information about late effects such as what late effects to expect and how to deal with late effects, indicating the importance of adequate information provision, starting at diagnosis and continuing throughout survivorship care [41, 42].
Strengths and limitations
This is the first cohort study on the presence, number and specific types of clinically relevant health conditions in relation to a wide range of psychosocial outcomes in long-term CCS. Major strengths are the unselected nationwide cohort, the detailed and reliable data regarding health conditions, and the comprehensive range of psychosocial outcomes covering emotional, social, cognitive and physical domains. This provided us with the opportunity to study the association between health conditions and psychosocial functioning in depth.
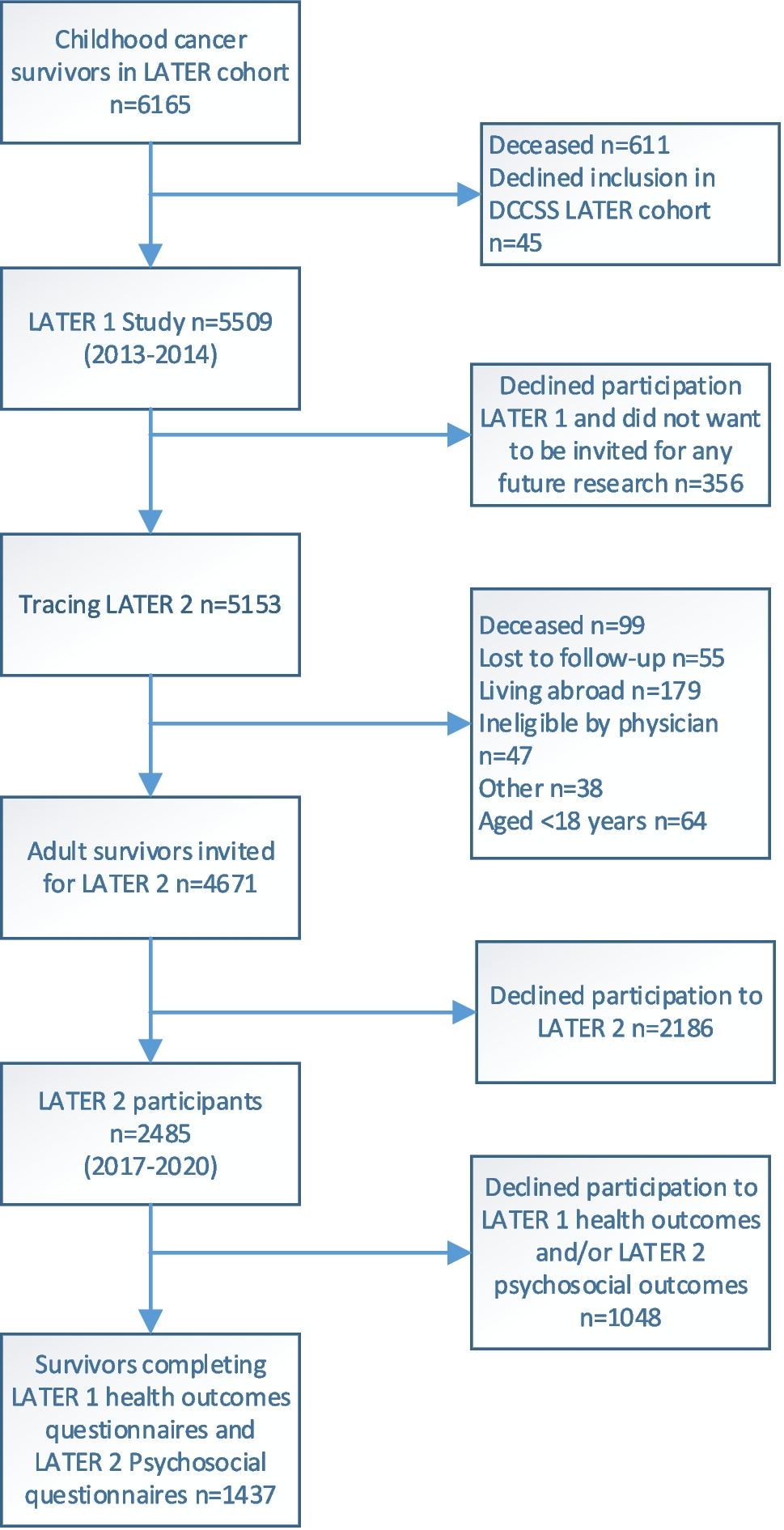
There are some considerations with the interpretation of the results. First, due to the time gap between the assessment of health conditions and psychosocial outcomes, changes may have occurred in CCS’ health status. While the vast majority of clinically relevant health conditions are permanent [5], CCS may have developed additional conditions in the meantime. Second, we have defined health conditions in various ways in our analysis (presence (yes/no), number, and specific types of health conditions). However, we did not assess the severity of health conditions, which might also affect psychosocial functioning in CCS, although we ensured the clinical relevance of all conditions. Additionally, health outcomes were self-reported and may not always be reported accurately. To mitigate this limitation, we validated the reported outcomes through self-reported medication use or by reviewing medical records. Third, even though this study had a large number of participants, some subgroups with specific types of health conditions were fairly small causing lower power to detect associations with psychosocial outcomes. Fourth, we have extensively examined the association between health outcomes and various psychosocial outcomes. Given the exploratory character of the study and the limited prior research on this topic, we opted for a moderately conservative correction for multiple testing to avoid overlooking potentially relevant associations between health conditions and psychosocial outcomes. Therefore, the possibility of false-positives should be taken into account when interpreting the results. Finally, this study included over half of the CCS invited for the LATER 2 study. We cannot rule out differences in health outcomes and psychosocial outcomes between participants and non-participants. However, we have not found important differences by diagnosis and treatment characteristics, and the presence of health conditions in these participants (45.2%, N = 1437) was in line with the presence in the total group that provided data on health conditions (46.4%, N = 3152) [5].

留言 (0)