Survey
We received 106 responses to the survey: 52 responses from individuals approaching the end of life or someone important to them, and 54 from health or social care staff. Demographic data are shown in Table 1.
Table 1 Demographic information and professional information for survey respondents, by groupThe 52 responses from people approaching the end of life or people important to them indicated that the individuals for whom they were responding had a range of conditions, including cancer (15, 29%), a long-term life-limiting physical condition other than cancer (24, 46%), dementia (4, 8%), a mental health condition (1, 2%) and another form of disability (3, 6%). Thirty of the 52 were people important to the person at the end of life, including family, friends or informal carers; just over half (16, 53%) of them had been assigned lasting power of attorney for health and welfare.
Around half of participants agreed or strongly agreed that they felt prepared for the conversation about EOLC when it started and that the people they spoke to were sensitive and caring. One third of participants agreed or strongly agreed they had a good understanding of services available to them and 35% agreed or strongly agreed that they felt confident that their preferences would be followed by clinicians and others providing care.
In terms of who is best placed to initiate a conversation, over half of participants felt that a member of a palliative care team specialised in EOLC, the person’s GP, someone important to the person approaching the end of life, or a member of staff at a hospital that the person has regular appointments with would all be appropriate.
Participants were asked to rate the importance of discussing and documenting various aspects of EOLC with health or social care staff. Based on percent selecting ‘Very important’, participants felt that their perspective on quality of life versus prolonging of life was highly important (85%), as were desired outcomes (85%) and specific treatments they would or would not like to receive (81%) (see Table 2). Relatively, a lower proportion of respondents rated discussing who should be present at death (56%) and preferred place of death (65%) as very important.
Table 2 Selected survey responses, by groupHealth and social care professionals
Health and social care professionals were asked similar questions to those asked of the first group, allowing comparison of some responses between groups. They recognised that several groups could be well-placed to initiate EOLC conversations – compared to people planning for EOLC and those important to them, the majority of health/social care professionals additionally indicated that another member of the general practice or community healthcare team, a member of social care staff, or the person approaching the end of life themselves would be appropriate (see Table 2). Just under half of respondents also selected a member of staff at a hospital that the person may not know so well as appropriate (see Table 2). Overall, health and social care professionals had more positive views about the appropriateness of most of the identified groups in initiating conversations, compared to people planning for EOLC and those important to them.
With regard to the content of conversations, nearly 90% of health and social care professionals rated ‘important outcomes’, and 80% rated ‘people’s views on the balance between prolonging life versus maximising quality of Iife’, as very important to discuss. Identifying who should be present at death was rated as very important by 61% of respondents, though discussing or putting in place legally binding arrangements appeared to be relatively less important for this group than for people planning EOLC and those important to them.
In terms of their own ability to discuss EOLC preferences with patients, over half of respondents strongly agreed with each of the statements that they had the right skills to start conversations and that they felt comfortable having those discussions. Only about a third of respondents strongly agreed with statements that they had access to the right tools and resources to have productive conversations and that they were confident in making treatment decisions when a patient has lost capacity.
When asked in an open-ended question what would be most helpful in identifying people approaching the end of life, having conversations about their EOLC preferences with them, or recording and sharing these preferences, one third of respondents mentioned having a nationally shared record across care services. In addition, several participants mentioned communication training, for example advanced communication to navigate difficult conversations and starting conversations with people not immediately at the end of their life.
Interviews
We conducted 21 initial stakeholder interviews with individuals from various backgrounds, including those with experience in palliative care practice and discussing plans for EOLC, and people from voluntary and campaigning organisations with an interest in this area. Additionally, we conducted 34 interviews with individuals who responded to the survey. Of the 34 interviewees, 14 were health or social care providers, 7 were individuals planning EOLC, and 13 were carers or people important to those at the end of life. The interviews provided rich detail of people’s experience with EOLC. Below we describe findings across the interviews relating to cultural, legal and educational issues, and challenges relating to service provision and resourcing constraints. We also discuss influences that support good EOLC planning communication and approaches that healthcare professionals said they found helpful in initiating discussions about EOLC planning.
Cultural, legal and educational barriers to implementation of good-practice standards
Interviewees shared their views on overall challenges in terms of ensuring that people’s preferences are known, shared, and acted on. People described their sense of how the palliative care approach was often at odds with a ‘culture of healthcare to cure’, to ‘intervene to save lives’.
‘If you can’t cure, it’s to control, and then [palliative care] feels like a failure, and that’s a mindset shift. You need to be able to hold in your head success being something other than cure or control.’ (Clinical academic in palliative medicine).
These contrasting mindsets could, in some participants’ views, deter both healthcare professionals and patients from opening conversations about EOLC options, and result in planning beginning later than optimal. The notion that it was countercultural to integrate enabling a good experience of death within good care was expressed across participants groups. One participant, for example, described the challenge of culture change in contexts such as emergency care where clinicians are tasked with assessing a situation very rapidly and making a decision in haste:
‘We’re in a way fighting against our historic traditional foundations of a lifesaving organisation. We’re trying to create a culture change.’ (Ambulance healthcare professional).
Relatedly, interviewees elaborated on how the culture of medicine was at times at odds with patient preferences. For example, some interviewees described situations where a person’s capacity was questioned simply because they did not agree with their clinicians, or chose to refuse treatment. These occurrences were, according to participants, not uncommon, despite clear legislation in England and Wales – the Mental Capacity Act – that deems that a person must be assumed to have capacity unless otherwise established. Another interviewee shared:
‘So, I’m very, very open with doctors about talking about [my advance care plan] and they didn’t like that, he said, “Oh no, no, no, let’s not talk about that now, let’s not discuss that”. My nurse really struggled with it at first, she was like, “Well, you know, we don’t need to talk about that”,’ and then when she became more aware of my story, she’s like, “OK I understand your thinking”. But I just find that I’m more open to talking about it than most healthcare professionals know how to deal with.’ (Individual planning EOLC).
Several interviewees brought up areas of confusion that made difficult EOLC situations even more challenging – for those planning EOLC and professionals alike. These included which advance planning documents are legally binding and which are not, as well as the status of documented preferences regarding attempted cardio-pulmonary resuscitation (CPR) as medical recommendations rather than legally binding documents (unless expressed in an Advance Decision). Participants also described lack of understanding surrounding the legal situation when a person loses capacity about the rights (or lack thereof) of family members, particularly in instances when the wishes of family members are not aligned with healthcare professionals seeking to act in the person’s best interest, or where there are differences of opinion regarding what the patient her/himself would have wanted.
‘[There is a] huge disjuncture between the law and medicine, how little doctors understand the law, how frequently doctors end up in court giving evidence and being cross-examined, and displaying their total ignorance about some of what are supposed to be the fundamentals of law in this country – to do with taking into account the person’s own values, wishes, feelings and beliefs, to do with the importance attached to autonomy, not simply to sanctity of life, and to do with basics like no, family are not the decision maker, the person giving the treatment is the decision maker.’ (Policy stakeholder).
Service provision and resourcing constraints on implementation of good-practice standards
Related to service provision, a particular challenge from professionals’ perspective was the tension between eliciting patient preferences and the reality of the availability of resources to meet people’s needs, and how conversations need to be bounded by system capacity (and communicated clearly) – particularly in less well-resourced areas.
‘I think one of the initial challenges was, historically, planning for end-of-life and palliative care has been focussed around cancer and there has been inequity with non-cancer conditions. So, services would have been developed in that way and commissioned from that perspective …. [Palliative care] covers all of the different service areas, so it’s part of a care pathway for all of those conditions. So, it’s taken quite a number of years for people to recognise that it’s part and parcel of many care pathways from a service provision perspective.’ (Manager in palliative care).
Influences on implementing helpful EOLC planning conversations
Influences identified as facilitating good conversations in practice included: sensitivity to what is important to someone; prioritising relationship-building; ensuring individuals feel in control; demonstrating empathy and compassion; and giving people the time they need (even when time is pressing). Others included the importance of courage in communicating difficult but important news, and the need to convey positive things that could arise from good planning without sugar-coating the prognosis.
‘You have to be prepared to say, “Going into hospital you might get better, but actually it’s a possibility you may not ever be well enough to come out of hospital and could die there”.’ (Healthcare professional in palliative medicine).
‘They [hospice workers] were so good, they provided me with the suction machine, they showed me how to use it, and they said, “This is how you use it, this is when you use it, but you know that it’s not going to stop him from dying but it will make him much more comfortable when he is dying”.’ (Carer).
Healthcare professionals discussed approaches they had taken in initiating conversations, and some shared frameworks and specific questions asked of patients and families to gain understanding of their perspectives. Some emphasised the importance of making known how the conversation would be documented and making clear if meeting preferences may not be possible due to resources or other reasons.
Most participants agreed that advanced communication skills were critical and that observing conversations was a valuable way of learning how to facilitate conversations better. They noted, however, that a focus on the completion of some advance planning documents could impede wider communication with an individual and preclude a full understanding of what is important to them.
Consensus-building
The consensus-building exercise took into account the main findings from the survey and interviews, specifically in areas where there would be meaningful learning or implications for EOLC. Findings from both datasets were used to identify key propositions about how practice might be improved, especially in relation to guidance about identifying people approaching the end of life, discussing with them their preferences for treatment and care, producing advance care plans, and ensuring that people’s preferences were accounted for in care provision. These were then formulated as (i) a series of statements and (ii) more detailed specifications of activities relating to some of those statements, which were considered through successive rounds of the consensus-building exercise.
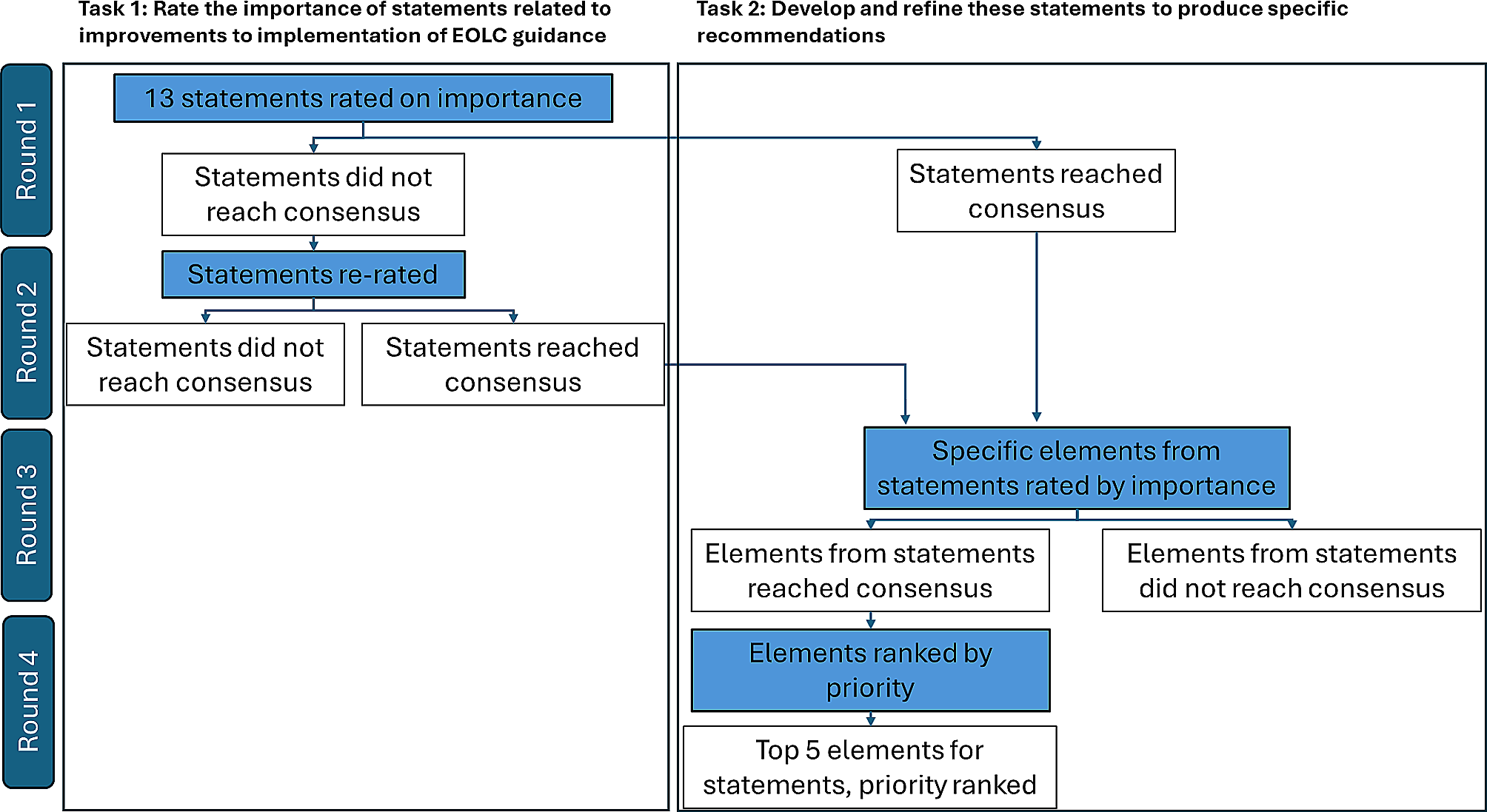
Rounds 1 and 2 – rating of statements
There were 475 participants in the first round of consensus-building (Table 3). In the first round, 11 of the 13 statements reached consensus. Two statements (statements 5 and 7 in Table 3) did not reach consensus and were therefore subject to a second round of rating. In this second round, 60% of respondents from the first round participated (n = 283). Neither statement 5 nor statement 7 reached consensus, with 60.8% and 64.9% agreement respectively after the second round (see Table 3).
Table 3 Final overall and group-level rates of agreement for consensus building statementsRounds 3 and 4 – Priority ranking of items relating to specific statements
All 475 participants from round 1 were invited to round 3 and 57% (n = 273) participated. Three statements that had achieved consensus in the first task of consensus-building were covered in rounds 3 and 4 in order to develop further specificity/granularity in recommendations for these areas:
statement 11 (‘A single, standardised approach to documenting and recording end-of-life treatment and care preferences is needed’).
statement 4 (‘We need to empower a wider range of people, including staff, people preparing for end-of-life and others, to initiate conversations about end-of-life treatment and care, for example by providing them with better skills and knowledge’).
statement 10 (‘Training on advanced communication skills should be provided to support healthcare professionals in initiating and conducting conversations about end-of-life treatment and care preferences’).
First, building on statement 11, participants were asked to rate the importance of incorporating various components into standardised documentation (using a nine-point scale, from 1 – Not important at all to 9 – Extremely important). All items reached consensus with mean ratings between 81.3% and 99.3%, including seven items with consensus above 95% (Table 3).
Second, building on statement 4, participants were asked to choose and then rank five groups of people (from a list of 11 groups) who should be prioritised in efforts to improve skills and knowledge. The top five groups selected, in order by highest to lowest rank, were: general practitioners; staff in care homes; palliative care staff; specialist nurses; and healthcare staff working in the community setting (Table 3).
Third, building on statement 10, participants were asked to choose and then rank the five most important topics (from a list of 10 topics) for advanced communication skills training. The top five topics selected, in order by highest to lowest rank, were: exploring what matters to the person and people close to them, and what concerns they might have; initiating conversations about EOLC; respecting people’s decisions about treatments they wish to receive when having conversations with them, in line with the Mental Capacity Act; facilitating and responding to questions, including signposting people to other sources of support; and talking to the person about illness progression, including prognostic uncertainty (Table 3).

留言 (0)