To our knowledge this is the first study to investigate and compare the perceptions of medication use and barriers and facilitators of appropriate medication use during palliative sedation, in eight European countries. We found distinct patterns of medication use, with perceptions of their use more in line with current EAPC recommendations [5] in the countries where palliative care services had been established longer (The Netherlands, Belgium, Germany, and the UK). Perceptions of the main barriers to the appropriate use of palliative sedation showed that lack of adequate knowledge and availability of certain medications in certain settings were considered as the main obstacles across all the studied countries, with the highest percentages of expert clinicians having this perception in Italy and Romania. It must be noted, however, that the observed differences in the patterns of medication use may have been influenced by differences between the practice of palliative and hospice care provision between the countries and the interpretation of the term ‘palliative sedation’, between the respondents from the different countries.
Palliative sedation can be indicated when patients with a terminal illness, experience refractory physical and/or psychological symptoms – and in some cases existential suffering- which cannot be adequately managed by other supportive and palliative treatment methods [15]. These symptoms include pain, dyspnea, delirium, agitation, anxiety and vomiting and palliative sedation may be indicated in 10–50% of the cases [16, 17]. According to the 2009 EAPC framework, benzodiazepines and, in cases of delirium, (additional) neuroleptics should be used primarily for achieving sedation [5], which is also recommended by guidelines in the Netherlands and Spain [18,19,20]. Among benzodiazepines, midazolam and among neuroleptics, levomepromazine are the medications primarily recommended [18,19,20]. Possible alternatives to midazolam are diazepam, lorazepam, clonazepam and flunitrazepam [15, 18,19,20,21]. Chlorpromazine, clotiapine, [22] and promethazine [21] are possible alternatives to levomepromazine, as described in the 2009 EAPC framework and the Italian, Spanish, Belgian and Dutch guidelines.
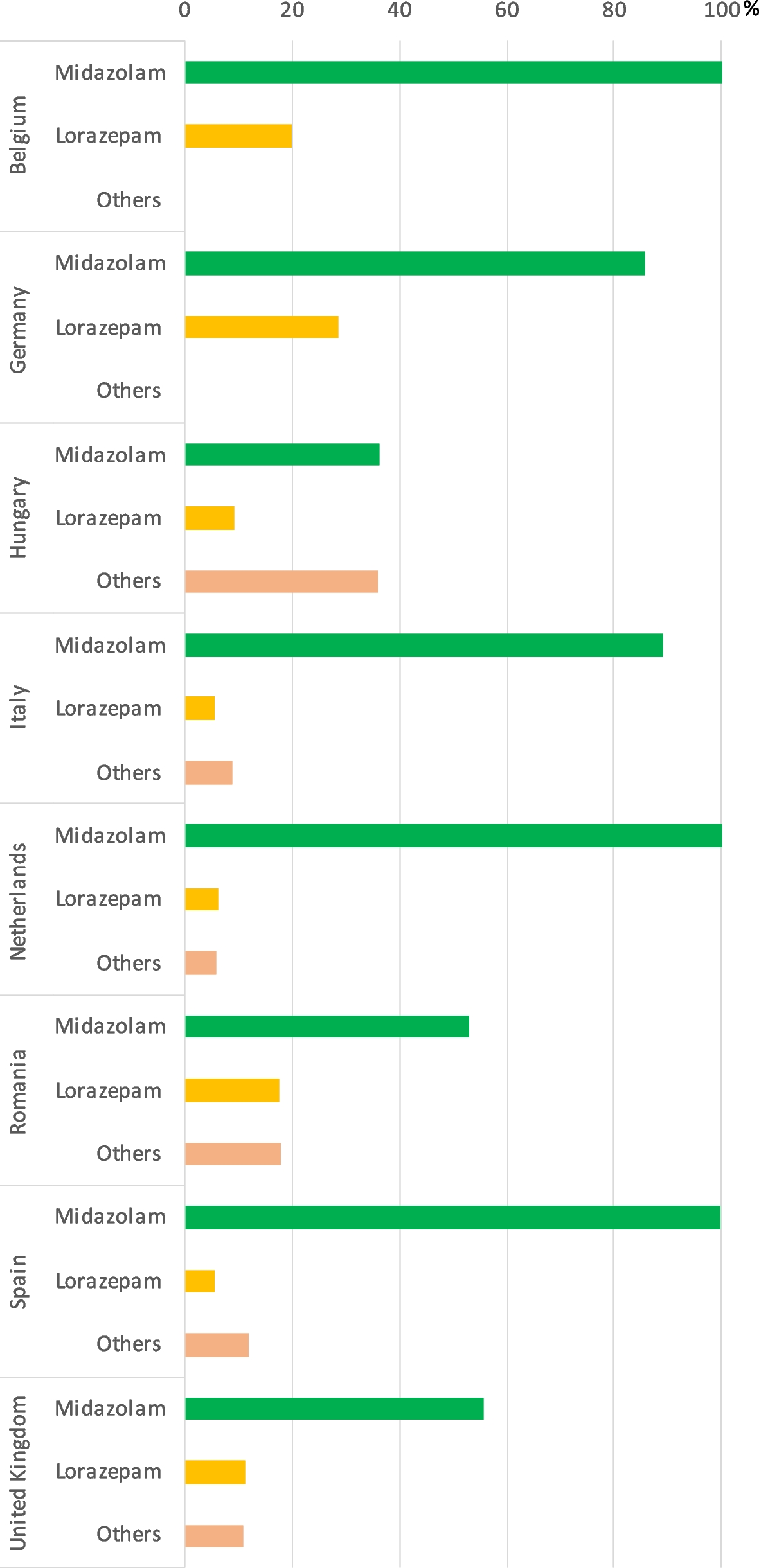
Our study showed that in line with the mentioned guidelines, midazolam was perceived to be used most frequently, i.e. “almost always”, in all eight countries, however, there were notable differences. The highest proportions with perceived midazolam use were mostly the Western European countries (The Netherlands, Belgium, and Germany) and South-European countries (Spain, Italy), while experts in the Central and Eastern European countries, like Romania and Hungary considered the primary use of midazolam much less frequent, with “almost always” use of midazolam being less than 40% in Hungary and similar to “other” less frequently used benzodiazepines. [23]. These perceived differences in the availability and use of midazolam may be explained by differences between the countries regarding the types of palliative and hospice care service provision in different settings as well as what medications can be prescribed and legally given at home [24,25,26]. In addition, the much more recent establishment of palliative care services – and concomitant guidelines- in the Central -European countries investigated in our study compared to countries where palliative care has been present for decades, like the Netherlands or the UK, could also have led to the observed differences [27]. According to a systematic review, availability of medications for palliative sedation at home are important, since it is both a feasible treatment option and an option for improving care for those who do not wish to be treated in a hospital setting [28].
In our analysis, the patterns in neuroleptic use were much less uniform among the countries, than for midazolam, since the primarily recommended levomepromazine [5, 18,19,20] was perceived to be used for palliative sedation “almost always” by less than half of the expert clinicians in the countries, the Netherlands, Spain, Germany, and the UK. The lower perception of the use of levomepromazine is supported by the EAPC recommendation, that midazolam is the first choice, when initiating palliative sedation and neuroleptics should mostly be used in cases of delirium or as a second line medication in combination with a benzodiazepine [5] Expert clinicians in Italy, Romania and Hungary did not report frequent perceived use of the first-line neuroleptic, levomepromazine, and mentioned “other medications” as being more frequently used. Knowledge, in general about the use of levomepromazine appeared to be lacking, which was demonstrated by the high proportion of key experts answering “don’t know” or leaving the question blank, when asked about levomepromazine’s perceived availability. The Hungarian guideline regarding palliative sedation does not specify the use of neuroleptics, which could explain the high number of “don’t know” answers [23].
Depending on the patient’s symptoms, co-medications may be administered during palliative sedation. Since pain and dyspnea are often cited as a refractory symptom, opioids may be given to complement treatment with sedatives [15]. However, the use of morphine should be used exclusively for the alleviation of pain and dyspnea and not as a sedative, as emphasized by the Dutch and Italian guidelines [18, 19, 21]. Although expert clinicians in most of the studied countries perceived the use of opioids to be relatively frequent during palliative sedation, the country, where expert clinicians perceived to be using them the most was in Hungary. In contrast, only 38% of the Dutch clinicians—in line with the mentioned guidelines- believed it to be used “almost always”. The observed difference in opioid use between the countries raises several questions: whether this was due to actual differences in the management of pain and dyspnea in terminally ill patients or to the inadequate assessment of pain by clinicians or that opioids – despite the national guidelines—were considered to be used instead of midazolam with the aim to sedate the patient.
Either way, our finding calls attention to the importance of the correct assessment of pain in terminally ill patients and to the importance of the use of opioid medications for the correct indications during palliative sedation.
According to the 2009 EAPC framework, “artificial hydration/nutrition therapy (….) should be individually decided through comprehensive evaluation of the patient’s wishes and the estimated benefits/harms” [5]. The ESMO clinical practice guidelines also stress the importance of decision making tailored to the individual patient’s needs, in consensus with the family members and the health care providers [15]. In contrast, the Belgian and Dutch guidelines state that administration of fluids is considered medically futile due to the terminal state of the patient’s illness when palliative sedation is deemed appropriate [15, 18, 22].
Reflecting the above-mentioned recommendations, both IV hydration and artificial nutrition were not perceived to be used frequently during palliative sedation in Belgium, the Netherlands, Germany, and the UK, in our study. South-European expert clinicians had a slightly different view: some frequency in IV hydration was perceived by clinicians in Spain, while clinicians in Italy reported the highest perceived use of IV hydration. The country where both IV hydration and artificial nutrition were considered to be used with notable frequency (about 30% “almost always”), was in Hungary. Although Hungarian palliative guidelines mirror the recommendations of the previously mentioned EAPC and ESMO [5, 15] guidelines, the perceived practice of hydration and nutrition in terminal patients appeared to show the opposite tendency. However, this phenomenon can partly be explained by specialized palliative care – and consequently palliative sedation- being available mostly in hospital settings, where the practice of artificial hydration and nutrition is more part of the routine practice in the care of patients than in the home setting. Similarly, the comparatively high perceived use of antibiotics in the UK could be due to the characteristics of the practice of palliative sedation; since palliative sedation is used intermittently to offer respite from suffering and not just near the end of life, this phenomenon may contribute to the higher perceived usage.
There is limited data regarding the factors that enable or impede the practice of palliative sedation. A study conducted in the UK investigated the ethical dilemmas hospice nurses faced during the administration of palliative sedation which concluded, that increasing the competence of nurses might facilitate the correct practice of palliative sedation [29]. Although palliative care services have been established longer in Western countries, like Belgium, lack of knowledge among GPs regarding correct palliative sedation practice and not being able to meet the needs of end-of-life care at home have been reported [30]. Corresponding with this study, we found, that lack of knowledge and unavailability of medications in certain settings were among the top four reasons perceived to be main barriers in the appropriate medication during palliative sedation—irrespective of the country- across all eight countries.
The perceived facilitators mirrored the perceived barriers to palliative sedation since improved education (to combat the barrier of lack of knowledge) and the availability of palliative care teams and availability of medications (to combat unavailability of medication and unavailability of a team specialized to perform palliative sedation) were perceived as the main facilitators of correct medication strategies during palliative sedation. The distribution of the top four reasons thought to be the main facilitators to the correct use of medication in palliative sedation showed that the education category reflects the need seen by experts to improve education on sedation medications at both the professional and the undergraduate levels.
These results therefore appear to emphasize the importance of education, possibly both at the graduate level at medical schools and at postgraduate levels as continuing medical education to educate clinicians on up-to-date evidence-based care regarding the medications-related guidelines for palliative sedation. Furthermore, studies on the practice of palliative sedation, like the present investigation, and subsequent measures aimed at informing those involved in health policy as well as the public. The results of these studies may also be important in improving the practice and acceptance of palliative sedation.
Limitations
Our study has several limitations. The study was conducted on a comparatively small sample of clinicians and the number and profiles of respondents per country differed, nor were the number of clinicians representative of the countries’ population, which could all have led to bias. Furthermore, the choice of respondents (who were invited to participate) could have led to bias and the answers given by the respondents were not actual documentations of the practice of palliative sedation in the given country, rather a subjective opinion, of how the practice was perceived, potentially leading to memory bias. The majority of the respondents were based in inpatient care (specialist palliative care in hospitals or hospices) and were physicians, and this thus, was a source of bias, furthermore, the inclusion of nurses could also have introduced bias. The combination of the 'very often' and 'always' categories may have influenced results, by artificially increasing the frequency. Finally, differences in the interpretation of categories of frequencies (almost always, very often, sometimes, rarely, almost never, not available (n/a) and the term ‘palliative sedation’ between the respondents as well as differences in the structure of palliative and hospice care, the availability of palliative and hospice care in different settings and the actual practice of palliative and hospice care between the countries could also have influenced our results and led to bias.
Nevertheless, the aim of the study was to obtain the perceptions regarding medication use in palliative sedation, which could be collected from the survey.

留言 (0)