In this nationwide, register based study we found that pain during the last week of life was registered in most patients dying of cancer (81%). It was also prevalent, although to a lower degree, in dementia (69%), heart failure (68%) and in COPD (57%). Severe pain was seen in 35% of all patients with cancer, and in 17–21% of patients with non-cancer conditions. Complete or partial pain relief was possible to obtain in most patients, as only 0,2% of the patients were not at all relieved.
Cancer-related pain
In our study, we conclude that pain, as well as episodes of severe pain were more frequently seen in patients dying of cancer, than in heart failure, COPD or dementia, which is a reminder of why the modern hospice movement focused on the needs of cancer patients in the early days [21]. Our results, with more than 80% of patients having occurrence of pain during the last week of life, show higher prevalence than previous studies with 55% of patients having pain [12]. This difference might be affected by the fact that pain has been measured at different time points and pain seems to increase towards end of life [13]. Moreover, temporal patterns are of great importance, as the intensity of pain varies throughout the day and is affected by circumstances such as pain in rest compared to movement, which could affect the pain prevalence reported in different studies [22]. Within oncology, a phenomenon of breakthrough pain is referred to. As described in a recent study by Mercadante, breakthrough cancer-related pain is a complex phenomenon that may change its presentation during the course of patients’ disease [23], which might affect the prevalence of pain in different studies. Patients may experience breakthrough pain differently, so rather than defining breakthrough pain as a phenomenon with a typical pattern, it is likely that the plural term of “breakthrough pains” is more adequate [23]. Breakthrough of pain, despite ongoing pain treatment, is more common in cancer- than in non-cancer conditions. This is, however, not an excuse for inadequate pain management in non-cancer conditions. Clinically, it is more likely that staff asks a patient with advanced cancer about pain, compared to patients with non-cancer diagnoses, which leads to a risk of insufficient pain treatment in the latter groups.
Pain in COPD and heart failure
The prevalence of pain in our study was 57% and 68% in COPD and heart failure, respectively. This is in agreement with other studies, although they show a considerable variation in figures from about 20 to 80% [24,25,26,27,28,29]. Reasons for different prevalence of pain in studies might be related to how pain is measured. Some studies only examine prevalence with a single yes/no question, while other studies rate pain intensities numerically or verbally and then report either all pain, including mild pain, or only moderate and severe pain [30]. Moreover, some studies use patient reported outcomes (PROs), whereas others rely on proxy measures, which may result in partly different figures [31, 32].
In COPD, some of the pain problems originate from the thorax [26], but also low back pain and chronic neck pain are common features [27]. In persons with heart failure, thoracic pain as well as abdominal pain originating from a swollen liver are commonplace [8]. Moreover, persons with COPD or hearth failure are often elderly, and in whom chronic muscle pain, as well as osteoarthritis are often seen [8]. In both groups, occurrence of pain was completely relieved in more than 70% of the cases in our study, and completely or partially relieved in more than 99% of the cases. However, the fact that 17% and 21% of the patients with COPD and hearth failure, respectively, had severe pain during the last week of life, shows that there is room for improvement, where an increased basic pain treatment would likely be most beneficial.
Pain in dementia
Persons dying from dementia with concomitant pain problems need attention. Pain is in this group of patients known to be overlooked and, when diagnosed, also undertreated and more difficult to follow up [33]. When dementia is the main diagnosis, most persons eventually lose their ability to communicate, which requires the staff to use non-verbal instruments such as Abbey Pain Scale, to assess pain by the means of typical pain behaviors [34]. Compared with cancer, dementia is more seldom associated with pain problems, still pain was registered in as many as 69% of the patients in our study, which underlines that staff should be aware of the need of knowledgeable symptom control. Moreover, behavioral and psychological symptoms of dementia (BPSD) are often seen as the main challenge in dementia care, as BPSD affects patients, the families, and the staff. BPSD include a range of neuropsychiatric disturbances such as agitation, aggression, depression, and apathy. Recent studies have shown that BPSD might be associated with unrelieved pain, meaning that if pain is well controlled, also the problems with BPSD reduces significantly [35,36,37].
Pain relief and opioid prescription
We found that he majority of patients with pain during the last week of life had complete relief of pain and most patients also had injectable opioids prescribed as needed. In Sweden, the goal is that all patients in end-of-life care have injectable opioids prescribed as needed, to enable good symptom control. Moreover, the Swedish National Board of Health and Welfare has defined prescription of injectable opioids in end-of-life care as a quality indicator, with a 98% target level as regards predictable deaths [38]. Thus, the high proportion of patients having pain relief and prescribed opioids as needed can be explained by these circumstances as pain relief is affected by the availability of opioids [39].
Strengths and limitations
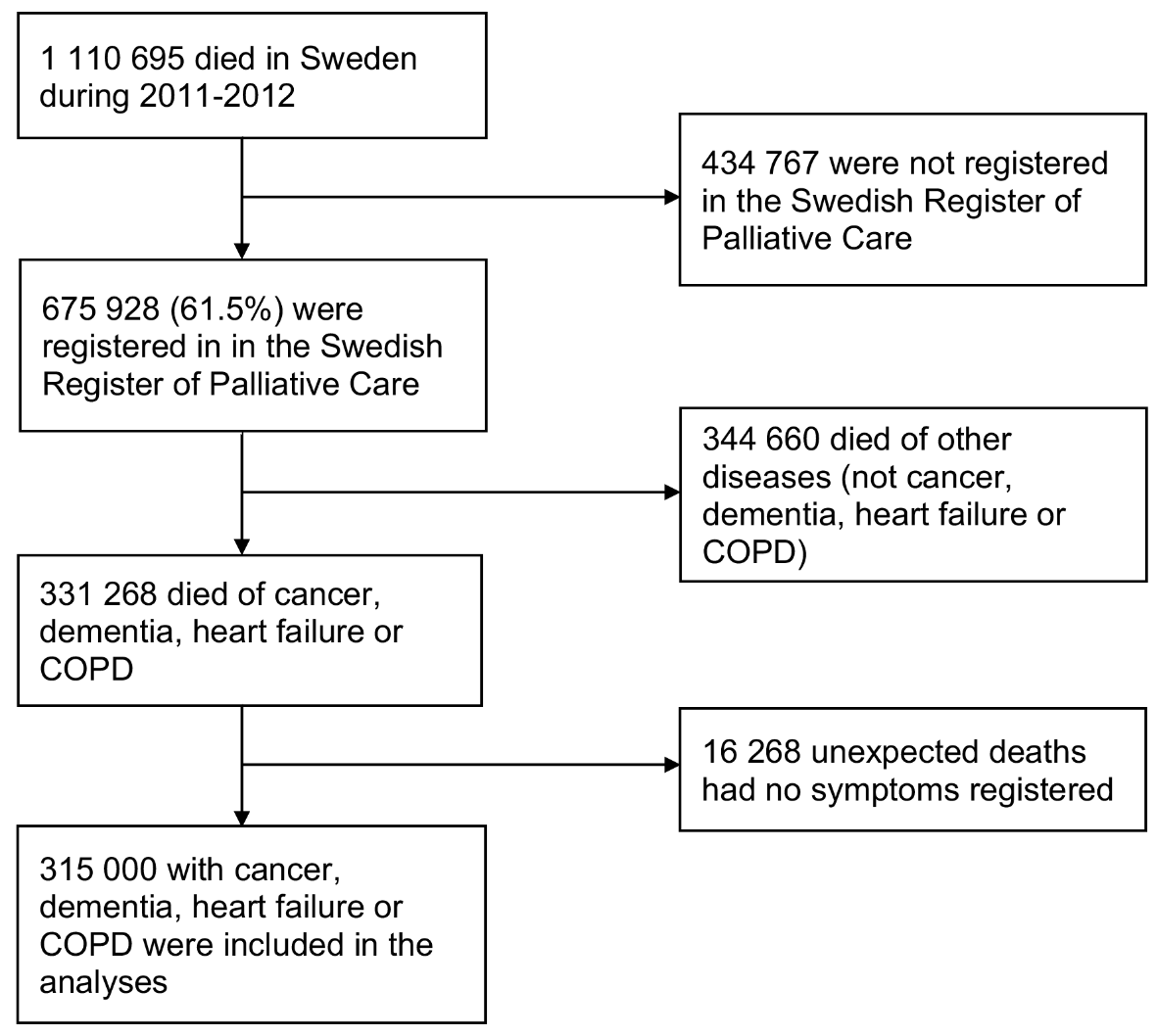
To the best of our knowledge, we here present the so far largest material on prevalence of pain during the last week of life, based on data from more than 300 000 persons. It is unique since pain was registered with the same questionnaire throughout, which makes the figures comparable between cancer and non-cancer diagnoses. While several prevalence studies are delimited to certain settings, e.g. to specialized palliative care, primary health care, nursing homes or acute hospital care [25, 26, 29], the prevalence of pain in this study is believed to have good potential for generalizability since our data cover all settings. Furthermore, the widespread use of the SPRC with its geographical representation from all parts of the country strengthens the external validity of our findings.
There are several limitations to our study. First, we do not know to what extent the underlying pain was preemptively treated, which may affect the proportion of people who experience significant pain. Further, adherence to agreed routines for data collection is a common problem for most registers, and the SRPC constitutes no exception [40]. Moreover, there are no instruments that are validated for symptom assessment in the imminently dying patient with lowered level of consciousness, which means that pain needs to be identified indirectly by the health care staff. Thus, when instruments were not used, the reporting was based on subjective judgments by the staff performing the registration. Moreover, pain assessment tools used in patients with dementia, such as the Abbey Pain Scale, might have inadequate psychometric properties in this population, such as validity, which can affect pain assessment negatively [41]. Consequently, symptom assessments to some degree depended on the level of knowledge, skills, and personal attitudes.

留言 (0)