
記住我
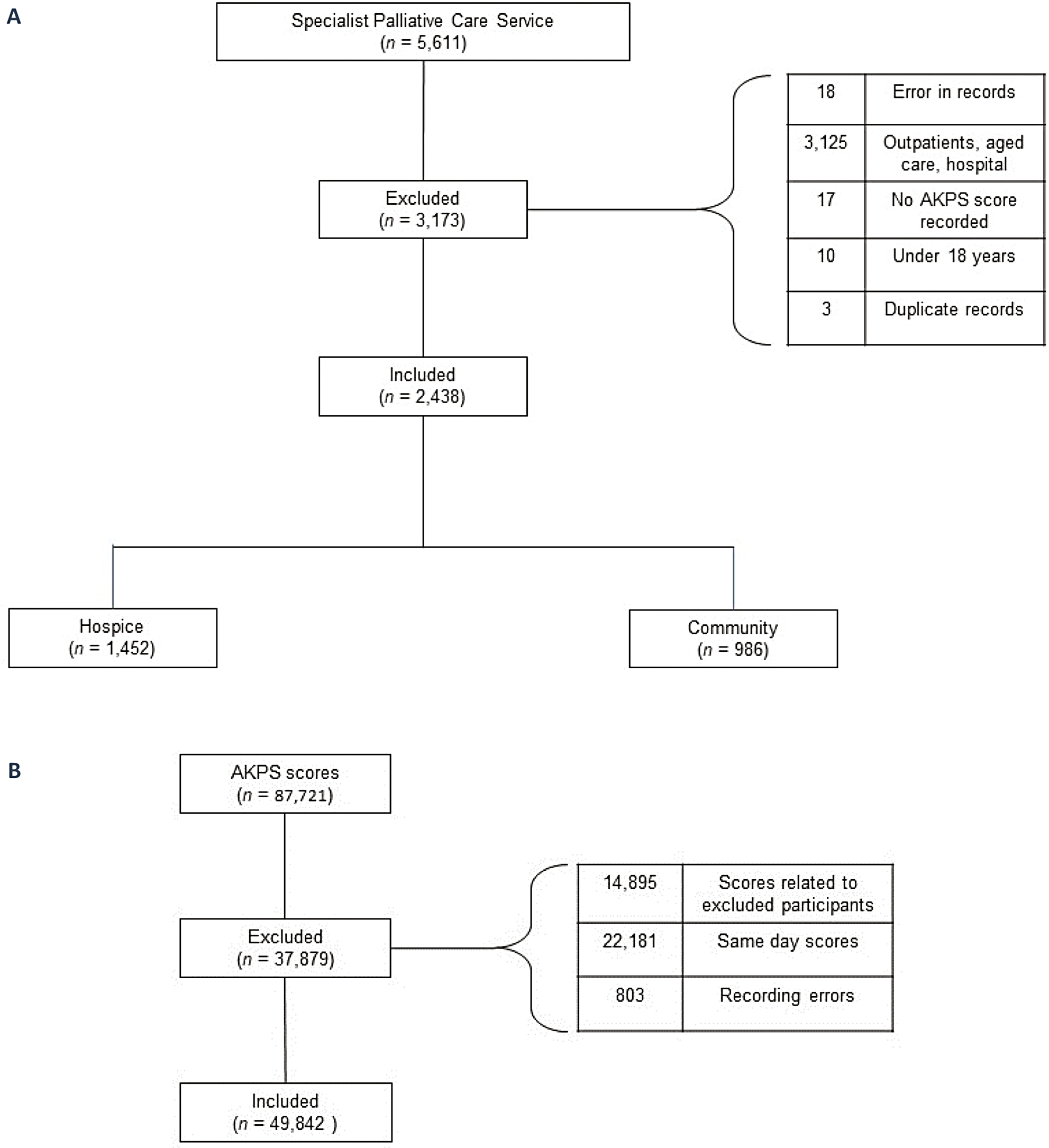
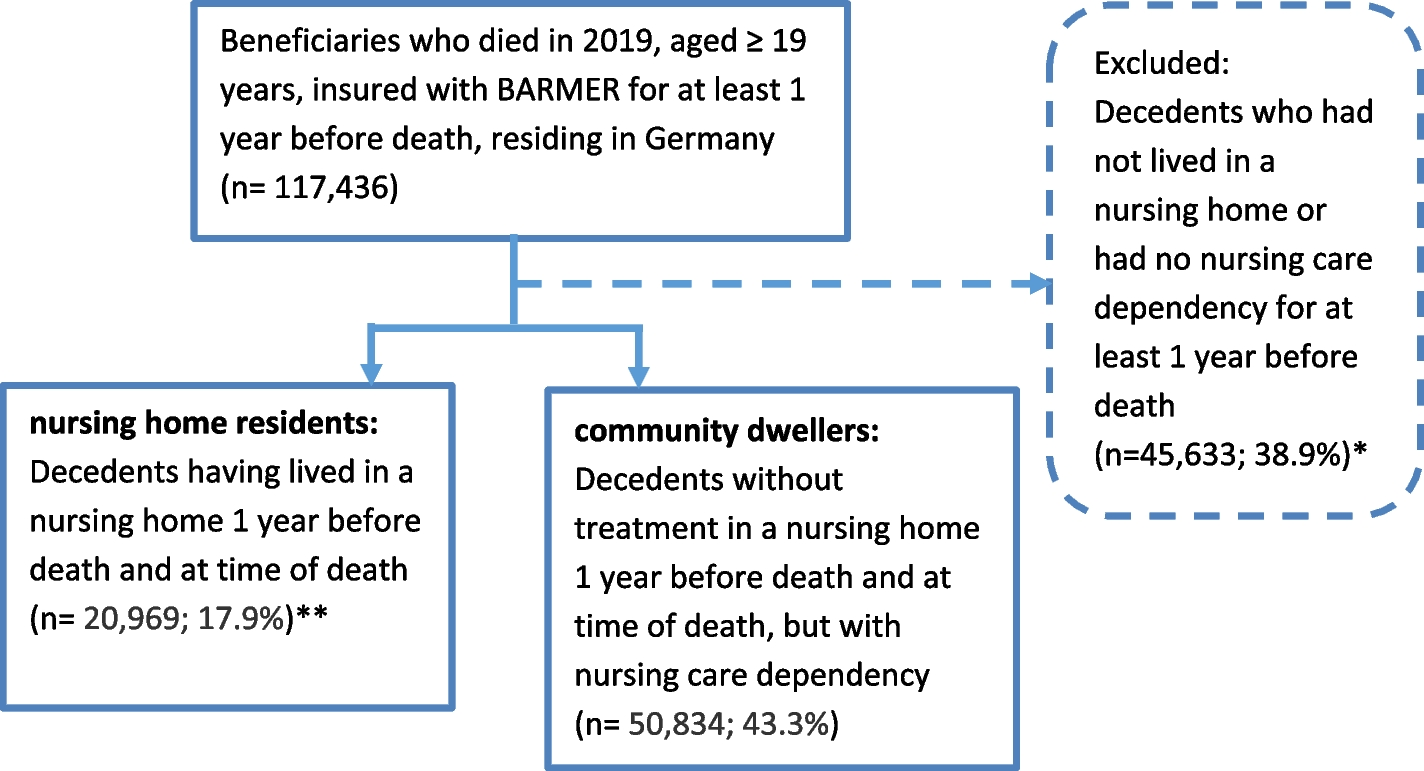




Of the 841 inpatients screened, 504 met the inclusion criteria and were eligible for review using SPICT™, with 171 (34%) being eligible for study enrolment. Of those eligible, 120 (108 inpatients and 12 carers; 40 respondents from each ward) agreed to participate (participation rate 70%). Fifty-one eligible inpatients did not complete consideRATE because: they were not approached (n = 10), off ward for any reason (n = 34), discharged home (n = 3), asleep (n = 2), unwell (n = 1) or declined without reason (n = 1). Table 3 shows participant characteristics.
Table 3 Demographics of participants who completed the consideRATE tool (n = 120)Ratings of care experienceTable 4 summarises data from the survey responses. Questions with the highest proportion of ‘very good’ responses were attention to symptoms (question 1), attention to feelings (question 2) and attention to what matters (question 4). Attention to patients’ affairs (question 6), attention to what you can expect (question 7) and attention to the physical environment (question 3) had lower proportions of ‘very good’ ratings (Table 4). Almost half (n = 57, 48%) of participants stated that the question about attention to patients’ affairs (question 6) ‘did not apply’ to their inpatient stay. All responses tended to be left-skewed, and median score was 3 (‘good’) for all questions.
Table 4 Patient (n = 108) and carer (n = 12) responses to the consideRATE survey (n = 120)Core elements ofquality care experienceOf the 532 free text responses analysed across 8 questions, four themes influenced experiences of care quality including: 1) Feeling supported, 2) Feeling informed and 3) Feeling heard, referring to provision of care; and 4) Navigating the clinical environment, referring to the environment in which care is provided (Fig. 1).
Fig. 1
Key elements of quality inpatient palliative care experience
Feeling supportedParticipants felt supported when the hospital clinical team assessed and managed symptoms promptly, offered emotional and practical support, and understood what mattered most to patients. Families provided emotional support and clarified information for inpatients throughout an admission.
Regular assessment and prompt symptom managementThe importance of timely symptom management, enabled by supportive care models and allied health input was highlighted. Participants described their distressing symptoms, and how they valued the clinical team regularly assessing symptoms and offering effective symptom management.
“When I was getting short of breath, I had a team of people around me. They are providing me with oxygen at home so I can manage for a bit there with my family. I feel so much better than when I came in and I have this ward to thank for it.” (Patient, Male, 78, malignant illness)
Allied health input and supportive care models that enabled good symptom management and improved quality of life were also valued.
“Mum has been struggling to swallow well and has been coughing on anything she drinks, the speech pathologist has been working with us to improve this as it is really impacting her life.” (Carer of Female, 93, non-malignant illness)
Participants spoke about the value of prompt symptom management. Some reported processes for charting medications, busy health professionals and understaffing resulted in delays in symptom management.
“Nurses paged the doctor at night to get medications charted and a cannula put in to help my vomiting. It isn't their fault, but it took a very long time so I was unwell for quite a while. It feels like there is a lot of understaffing hospital wide.” (Patient, Female, 61, non-malignant illness)
Receiving practical and emotional support from health professionalsClinical teams’ provision of emotional and practical support reflected participants’ perception of how respectful clinicians were.
“I feel it has been very respectful, I always receive support I am never left alone when I am upset or worried.” (Patient, Male, 68, malignant illness)
Most appreciated the clinical teams’ emotional support after receiving distressing news or organising practical support at home:
“I am seeing the social worker, psychologist and kidney supportive care - the nurses are very supportive too, I've had difficult news this week.” (Patient, Male, 49, non-malignant illness)
“The social worker is helping me find a nursing home, this is important because I need more help and support, I can't be at home. (Patient, Male, 70, non-malignant illness)
However, a few participants described situations where they felt unsupported as they were given difficult news alone.
“You shouldn't tell people difficult news by themselves or without checking with them if they would like some support - always make sure they have the option of a support person so they aren't left alone …. it’s important to remember that these are people with lives and families.” (Patient, Male, 40, malignant illness)
Supporting what matters to inpatientsParticipants appreciated clinicians' paying attention to what mattered to them. This was enabled by checking in with participants:
“There have been people who have checked in on me to make sure I'm not just lying here thinking about things. They offer magazines and talk to me.” (Patient, Female, 78, malignant illness)
Participants also appreciated clinician’s being respectful of what matters to the inpatient and family and supporting future care planning.
“The ACP [advance care planning] nurse came to see me - I have done my decision maker documents. It’s a good service to have someone checking in about this sort of paper work, you don't always know what to do with it.” (Patient, Female, 96, non-malignant illness)
However some participants recognised that health professionals did not always prioritise what matters to them in the busy acute care environment.
“They’ve got a job to do. It would be nice and it makes it easier when there is a focus on what matters to you but I understand there are other priorities to focus on like treatment plans, processes and procedures.” (Patient, Male, 74, non-malignant illness)
The role of families in providing supportParticipants confirmed the vital role of family members in providing emotional support, which could reduce the need for emotional support provided by clinicians.
“I get a lot of emotional support from my family.” (Patient, Female, 46, malignant illness)
Many family members provided support to the participant by being an intermediary to communicate care plans to participants and facilitate their understanding of the care.
“They mostly talk to my daughter who helps me understand what is happening.” (Patient, Male, 81, non-malignant illness)
Feeling informedMost participants appreciated clinical teams who provided regular, honest information about day-to-day care planning and expectations of the future. This enabled participants to understand their treatment and make decisions about care. When health professionals did not inform participants of their care or used technical language, participants felt disappointed and felt clinical teams were disjointed and siloed.
Providing honest and regular informationParticipants valued being regularly informed with up-to-date information by their clinical team and having opportunities to ask questions and clarify information.
“I can't fault the care and I feel like I have been informed by all the people who come to see me, I am kept up to date, the communication has been open and I can clarify what I need to.” (Patient, Male, 71, malignant illness)
“They always clarify if we understand what they're saying. They [my family] are always involved by staff and feel they can ask questions. It has made it easier for them to accept/understand what's going on with me.” (Patient, Female, 41, malignant illness)
Participants appreciated honesty when they asked about future expectations of their illness so they could be prepared for the future.
“I appreciate honesty so I ask the tough questions. It's not always easy to hear the answers but I want to be prepared.” (Patient, Male, 66, non-malignant illness)
When health professionals took the time to speak openly and explain the overall care plan, it enabled participants to make informed decisions about their care.
“Lots of people have been involved in Mum's care - I have found talking to palliative care helpful to bring it all together and understand the overall plan.” (Carer of Female, 75, malignant illness)
Participants noted the difficulties they experienced when clinical teams do not provide clear communication, contradict each other, or show a lack of integrated care planning and provision.
“It fluctuates and can be disjointed. Doctors can contradict each other and vary depending on who's in charge. I don't really understand the global plans because there are so many teams involved - I feel disappointed that there is a lot of "lets watch and see how it goes". (Patient, Male, 63, malignant illness)
Feeling heardGood quality care experience was influenced by health professionals listening to participants’ physical and spiritual concerns. Valuing and acknowledging participants’ illness and symptom expertise was important for shared decision making. Feeling heard about preferences for future care was vital to the experience of good quality care.
Listening to physical and spiritual concernsListening to and respecting participants’ spiritual beliefs when making decisions about care was valued and influenced the perception of good quality care.
“I believe in God - the doctor I was talking to about my faith, he listened to me. It may not have been his belief but he sat and listened. The people that work here are a gift - the care has been magnificent.” (Patient, Male, 78, malignant illness)
Participants spoke about their symptom and illness expertise and the importance of being involved in the decision making around diagnostics and the care process. Listening to participants when they expressed symptom and illness concerns enabled participants to feel cared for and confident in the clinical team.
“I am a complex, long-term patient because of my kidney failure. I have been in hospital a lot. It can be frustrating when you feel you're not being listened to about what you think is wrong with you and it can take a lot of time to get to the bottom of it. I feel like I wasn't believed and, in the end, what I suspected was wrong with my back has shown to be correct on the imaging. I understand I am not a professional and appreciate there are processes and procedures, but I do know my body and as I said, I have been in and out of hospital over the years a lot with issues with my health. Sometimes it feels like my voice isn't heard.” (Patient, Female, 44, non-malignant illness)
For this reason, participants valued the opportunity to complete the PREM tool:
“I've really appreciated being asked about my experience - I have had a good experience but it is nice to be spoken to about it like this and be able to give feedback to improve care.” (Patient, Female, 61, non-malignant illness)
Feeling heard about care preferences if their illness worsensParticipants expressed the importance of being and feeling heard about preferences for care if their illness worsened. The focus on quality of life and not being burdensome to family was viewed to be important.
“I've spoken to my doctors about what I want if my illness gets worse like what is happening now. I don't want to suffer. We had a family meeting and the discussion was open and focused on what I wanted from here. Right now I feel like my quality of life is poor. I'd like to focus on comfort and I expressed that. I know they are going to withdraw the dialysis and I understand that I won’t have a long time left from there but I will be kept comfortable.” (Patient, Male, 76, non-malignant illness)
Many spoke about completing not for resuscitation documents with their doctors and used this as an opportunity to discuss preferences for a quality-of-life focus if their illness worsened.
“My quality of life is most important to me. I know my family want me to prolong my life and have as much time as possible but I don't want to live if my life isn't quality. I don't want to be a burden on my family. I have completed a not for resuscitation document with my doctors so that has been discussed a bit then.” (Patient, Male, 75, non-malignant illness)
Navigating the clinical environmentThis theme reflected the realities of receiving care within an acute environment and its impact on care quality. Health professionals’ attention to light, temperature and noise levels impacted participants’ health and wellbeing. A lack of access to television and kitchen appliances removed comfort and connection. Being in bays with other inpatients also influenced participants’ inpatient experiences.
Attention to light, temperature and noise level is appreciatedParticipants understood the busy nature of the hospital when tending to unwell inpatients resulted in noise.
“It is loud and busy in here and there are lots of confused people but I understand this is a hospital and people are quite unwell.” (Patient, Male, 86, malignant illness)
However, participants appreciated when healthcare providers were attentive to light, temperature and noise, as this was important for their comfort and wellbeing.
“The air conditioning feels very dehydrating - it is all the perfect storm for a migraine which I have suffered from for a long time. I feel people should be asked about this on admission.” (Patient, Female, 61, non-malignant illness)
Lack of access to home comfortsParticipants spoke about the lack of access to television, noting televisions provided connection to the world, a way to pass time while in hospital, and enabled a distraction from living with serious illness.
“You can't watch the news to see what is going on because there are no TVs - I've already missed so much this year with being unwell. It's not fair to have nothing to watch to give you some kind of pleasure…People sit in their room all day listening to their own thoughts.” (Patient, Female, 73, non-malignant illness)
A lack of access to simple kitchen appliances removed a sense of comfort, limited independence and detracted from a participant’s sense of self.
“It would be really good to have access to a kettle to make a cup of tea, sometimes you don't want to bother the staff …. but it can be something small like that that is comforting and makes you feel human, just enjoying a cup of tea.” (Patient, Female, 44, non-malignant illness)
Receiving care within four bedded baysParticipants noted their appreciation for ancillary staff and attention to cleanliness and hygiene when sharing common areas with other inpatients, although their expectations were not always met.
“The toilet hasn't been cleaned properly from a man in the bay preparing for a colonoscopy.” (Patient, Female, 78, malignant illness)
Preferences for bays with multiple inpatients varied. Some participants valued being with others for social connection.
“I'm a social person, not private - I like having the curtains pulled back and chatting.” (Patient, Female, 71, malignant illness)
However, some struggled with the lack of privacy due to their usual living arrangements.
“The lack of privacy is very hard when you're unwell in these 4 bed rooms. I'm not used to it, I live alone.” (Patient, Female, 75, non-malignant illness)
留言 (0)