
記住我
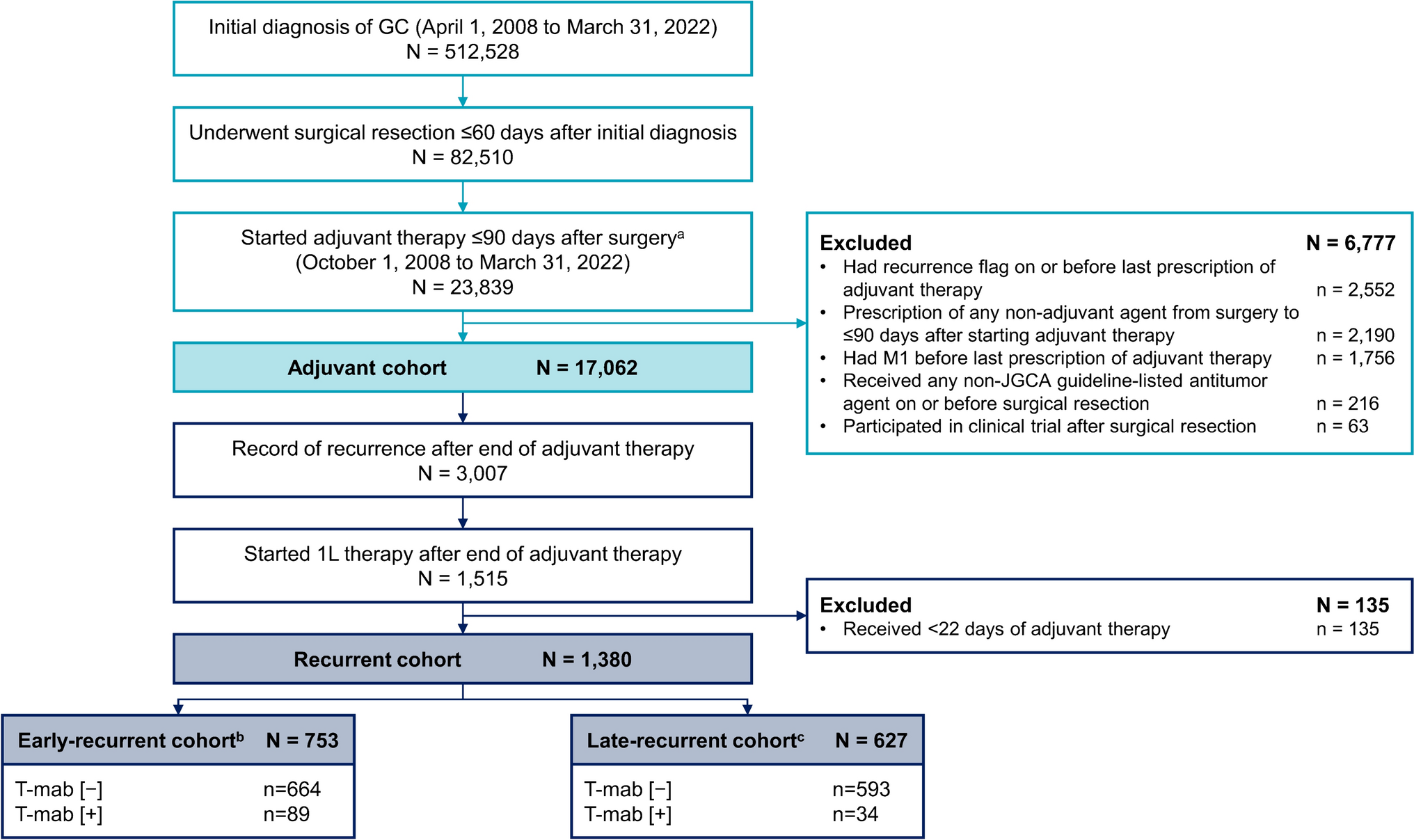


During the study period, 512,528 patients had a confirmed GC diagnosis, of whom 82,510 underwent surgical resection within 60 days of the diagnosis (Fig. 1). In total, 17,062 patients aged ≥ 20 years started JGCA guideline-directed adjuvant therapy on or after October 1, 2008 and were included in the adjuvant cohort. Of 3007 patients with recurrence after the end of adjuvant therapy, 1380 patients were included in the recurrent cohort; 753 patients had early recurrence and 627 patients had late recurrence.
Fig. 1
Patient flow. 1L first-line, GC gastric cancer, JGCA Japanese Gastric Cancer Association, T-mab/T-DXd [ − ] with no history of trastuzumab or trastuzumab deruxtecan treatment, T-mab/T-DXd [ + ] with a history of trastuzumab or trastuzumab deruxtecan treatment. aAged ≥ 20 years at start of adjuvant therapy; bStarted post-recurrent 1L therapy ≤ 180 days after end of adjuvant therapy; cStarted post-recurrent 1L therapy > 180 days after end of adjuvant therapy
Demographic and hospital information for patients were generally similar across the three age groups in the adjuvant cohort (Table 1) and in the T-mab/T-DXd [ − ] group of the recurrent cohort (Table 2). However, the prevalence of some comorbidities tended to be higher in patients aged ≥ 75 years than in younger patients in both cohorts. In the T-mab/T-DXd [ − ] group of recurrent cohort, the most common metastasis site was peritoneal or ascites, with this proportion being higher in the late versus early recurrent cohort. The demographic and hospital information for patients in the T-mab/T-DXd [ +] group of the recurrent cohort are summarized in Supplementary Table S3.
Table 1 Patient demographics and hospital admission information in the adjuvant cohortTable 2 Patient demographics and hospital admission information in the recurrent cohort among patients in the T-mab/T-DXd [−] groupAdjuvant therapy patternsAcross all three time periods, the most common adjuvant therapy regimen was S-1 (Fig. 2). The proportion of patients treated with S-1 decreased over time from 95.7% during October 2008–May 2016 to 77.7% during June 2016–August 2019 and 65.0% during September 2019–March 2022. The proportion of patients treated with fluoropyrimidine plus oxaliplatin combination regimens increased from 2.8% during October 2008–May 2016 to 16.7% during June 2016–August 2019 and 15.0% during September 2019–March 2022 after these regimens were recommended by the JGCA guidelines in June 2016 [2]. The proportion of patients receiving DS adjuvant therapy also increased from 1.5% and 5.5% during October 2008–May 2016 and June 2016–August 2019, respectively, to 20.0% in September 2019–March 2022 after this regimen was recommended in the JGCA guidelines in September 2019.
Fig. 2
Adjuvant treatment patterns by time period in the adjuvant therapy cohort (N = 17,062). CapeOX capecitabine plus oxaliplatin, DS S-1 plus docetaxel, S-1 tegafur/gimeracil/oteracil potassium, SOX S-1 plus oxaliplatin
The median duration of each adjuvant regimen generally remained similar across the three treatment periods, although SOX had a slightly lower median duration in the second time period versus the first and third periods (7.8 vs 10.0 and 10.2 months, respectively; Table 3).
Table 3 Duration of adjuvant therapy for gastric cancer according to adjuvant therapy start date in the adjuvant cohort (N = 17,062)During September 2019–March 2022, the proportion of patients who received S-1 was higher among patients aged ≥ 75 years (78.2%) than in those aged < 65 or 65–74 years (55.0% and 60.2%, respectively; Fig. 2). In contrast, the proportion of patients treated with SOX, CapeOX, or DS was lower in patients aged ≥ 75 years (6.3%, 3.4%, and 12.2%, respectively) than in those aged < 65 years (13.0%, 4.8%, and 27.2%, respectively) or 65–74 years (11.6%, 6.2%, and 22.0%, respectively).
Post-recurrent treatment patternsIn the T-mab/T-DXd [ − ] groupIn the T-mab/T-DXd [ −] group of the early-recurrent cohort, the most common post-recurrent first-line regimens (in > 10% of patients) were paclitaxel plus ramucirumab (34.0%), CapeOX (17.0%), and nab-paclitaxel plus ramucirumab (10.1%; Fig. 3a, Table 4). Among patients who received these common regimens, a higher proportion of the patients who received paclitaxel or nab-paclitaxel plus ramucirumab had peritoneal metastasis or ascites at baseline compared with those who received CapeOX (31.4% and 35.8% vs 15.0%, respectively; Supplementary Table S4). In the late-recurrent cohort, the most common first-line regimens were SOX (26.3%), SP (15.3%), CapeOX (14.0%), S-1 (13.2%), and paclitaxel plus ramucirumab (10.8%; Fig. 3b, Table 4). In sensitivity analyses, first-line therapy patterns remained similar when early versus late recurrence was defined as first-line treatment started ≤ 210 versus > 210 days after adjuvant therapy (Supplementary Table S5) and when the definition of regimen end was defined as 90 days (Supplementary Table S6).
Fig. 3
Treatment sequence in T-mab/T-DXd [ −] group of the recurrent cohort with a early recurrence (≤ 180 days from end of adjuvant therapy) or b late recurrence (> 180 days from end of adjuvant therapy). 1L first-line, 2L second-line, 3L third-line, 5-FU 5-fluorouracil, CapeOX capecitabine plus oxaliplatin, DS S-1 plus docetaxel, DTX docetaxel, FLN folinic acid, FTD/TPI trifluridine/tipiracil, FOLFOX folinic acid plus 5-fluorouracil plus oxaliplatin, IRI irinotecan, nab-PTX nab-paclitaxel, NIV nivolumab, PEM pembrolizumab, PTX paclitaxel, RAM ramucirumab, S-1 tegafur/gimeracil/oteracil potassium, SOX S-1 plus oxaliplatin, SP S-1 plus cisplatin, T-mab/T-DXd [ −] with no history of trastuzumab or trastuzumab deruxtecan treatment, T-mab/T-DXd [ +] with a history of trastuzumab or trastuzumab deruxtecan treatment, XP capecitabine plus cisplatin
Table 4 Post-recurrent first-line treatment patterns in T-mab/T-DXd [ −] group of the recurrent cohortIn the early-recurrent cohort, 596 patients discontinued first-line therapy or died, of whom 333 (55.9%) received second-line therapy (Fig. 3a). The most common second-line regimens were paclitaxel plus ramucirumab (29.4%) and nivolumab (29.1%). Among 119 patients who received third-line therapy, the most common regimens were nivolumab (42.9%), irinotecan (21.8%), and paclitaxel plus ramucirumab (14.3%).
In the late-recurrent cohort, 524 patients discontinued first-line therapy or died, of whom 289 (55.2%) received second-line therapy (Fig. 3b). The most common second-line regimens were paclitaxel plus ramucirumab (39.1%), nab-paclitaxel plus ramucirumab (15.2%), and nivolumab (12.5%). Among patients who received third-line therapy (n = 117), the most common regimens were nivolumab (54.7%), irinotecan (12.0%), and paclitaxel plus ramucirumab (10.3%).
The median duration of first-line therapy was similar in the early- and late-recurrent cohorts (4.6 vs 4.9 months; Table 4). The overall treatment duration (from the start of first-line therapy to end of the last line of therapy) was also similar in patients with early and late recurrence (median 9.0 vs 9.5 months). The proportion of patients who received second-line therapy was 55.9% and 55.2% in the early- and late-recurrent cohorts, respectively. When treatment durations were assessed in patients who started before and after October 2015, patients who started first-line therapy before October 2015 had numerically shorter median durations of first-line therapy and overall treatment in the early-recurrent cohort versus the late-recurrent cohort (first-line therapy, 3.5 vs 4.9 months, respectively; overall treatment 7.6 vs 10.0 months, respectively). In patients who started first-line therapy after October 2015, the median treatment durations were similar between the early- and late-recurrent cohorts (first-line therapy, 4.6 vs 4.9 months, respectively; overall treatment, 9.3 vs 9.5 months, respectively; Supplementary Table S7).
In the early-recurrent cohort, the median duration of first-line therapy for the most common regimens (i.e., paclitaxel plus ramucirumab, CapeOX, and nab-paclitaxel plus ramucirumab) was similar (5.0, 4.6, and 4.9 months, respectively; Table 4). However, the median overall treatment duration was numerically longer with CapeOX (11.9 months) than with paclitaxel plus ramucirumab and nab-paclitaxel plus ramucirumab (8.8 and 6.5 months, respectively), and the rate of first- to second-line transition was numerically higher with CapeOX (69.8%) than with paclitaxel plus ramucirumab (52.8%) and nab-paclitaxel plus ramucirumab (44.8%).
In the late-recurrent cohort, the median duration of first-line therapy and overall treatment was similar among the most common regimens, ranging from 4.9 to 5.6 months and 8.9 to 10.5 months, respectively (Table 4). However, the rate of first- to second-line transition was numerically lower with S-1 (38.2%) and paclitaxel plus ramucirumab (50.0%) than with fluoropyrimidine plus platinum regimens (60.4% for SOX, 66.7% for SP, and 58.7% for CapeOX).
First-line treatment patterns in the three age groups were generally similar in the early- and late-recurrent cohorts, but in the late-recurrent cohort, the median overall treatment duration was shorter in patients aged ≥ 75 years than in those aged < 65 years or 65–74 years (7.5 vs 10.4 and 9.5 months, respectively; Supplementary Table S8). The proportion of patients receiving first-line S-1 therapy in the late-recurrent cohort was higher in older versus younger patients (22.5% vs 5.4% and 12.5%, respectively), while the proportion of these patients who received SOX was slightly lower in older versus younger patients (20.6% vs 26.2% and 29.8%, respectively; Table 5).
Table 5 Post-recurrence first-line treatment regimens in T-mab/T-DXd [ −] group of the recurrent cohort by age groupIn the T-mab/T-DXd [ +] groupAmong 89 patients with early recurrence in the T-mab/T-DXd [ +] group, 73 (82.0%) received T-mab as part of their first-line regimen (Supplementary Fig. S2a). The most common first-line regimens were capecitabine plus cisplatin (XP) plus T-mab (49.4%), CapeOX plus T-mab (16.9%), and paclitaxel plus T-mab (10.1%).
In the late-recurrent cohort, 27 of 34 patients (79.4%) received a T-mab-containing first-line regimen (Supplementary Fig. S2b, Supplementary Table S9). In these patients, the most common first-line regimens were XP plus T-mab (41.2%) and SP plus T-mab (11.8%). The median durations of first-line therapy, overall treatment, and the first- to second-line transition rates for all first-line regimens are presented in Supplementary Table S9.
留言 (0)