
記住我




A 52-year-old male (height, 160 cm; weight, 50 kg; body mass index, 19.5 kg/m2) with intellectual disability was scheduled to undergo intrathecal baclofen pump insertion under general anesthesia to treat lower limb spasticity. Five years previously, the patient was diagnosed with HHH syndrome by genetic testing after recurrent epileptic seizures and hepatic encephalopathy. The patient was treated with lactulose (36 g/day), magnesium oxide (990 mg/day), and lacosamide (100 mg/day) for constipation and epilepsy and regularly consumed a low-protein diet supplemented with arginine (6 g/day). His serum ammonia levels were normally around 40–60 µg/dL (normal value, 12–66 µg/dL), with occasional elevations (100–150 µg/dL). The patient had undergone a colectomy for sigmoid cancer under general anesthesia without any complications at another hospital one year previously. Preoperative laboratory data showed normal liver and kidney function, and the serum ammonia level was 44 µg/dL. A preoperative diet (36 kcal/kg/day, 1.2 g/kg/day of protein) was provided until an evening meal the day before surgery. Fluid intake was maintained for up to 3 h before surgery, and lactulose, lacosamide, and arginine were continued until the morning of surgery.
In the operating room, the patient was monitored with electrocardiography, invasive arterial blood pressure, pulse oximeter, capnography, bladder temperature, and bispectral index. General anesthesia was induced with propofol 50 mg and fentanyl 50 µg. Thirty milligrams of rocuronium were administered to facilitate tracheal intubation. Anesthesia was maintained with oxygen 45%, desflurane 4%, and remifentanil 0.10–0.16 µg/kg/min. Hemodynamics were maintained with an occasional bolus of ephedrine 4 mg and continuous infusion of phenylephrine 0.3–0.5 mg/h. Sodium bicarbonate Ringer solution was administered during anesthesia. The surgery was completed without any complications. Intrathecal baclofen was administered at a dose of 20 µg/day. Nine minutes after discontinuation of anesthesia, the patient regained consciousness, and the tracheal tube was removed in the operating room. The duration of surgery and anesthesia was 106 and 228 min, respectively. The total intake was 1200 mL of sodium bicarbonate Ringer solution. During anesthesia, serum ammonia levels ranged from 27 and 46 µg/dL, and blood glucose levels ranged from 100 to 133 mg/dL. The patient was transferred to a high-care unit for postoperative monitoring.
The serum ammonia levels during the postoperative period are shown in Fig. 1. On postoperative day (POD) 1, the serum ammonia level mildly increased to 73 µg/dL. There were no symptoms suggestive of metabolic decompensation, such as nausea, vomiting, poor appetite, or decline in consciousness. Postoperative pain was well-controlled with acetaminophen 300 mg/day and loxoprofen 60 mg/day. The patient was transferred to the general ward, and a low-protein diet and regular oral medications were recommenced on the morning of POD 1. In addition to his medication, sodium picosulfate solution was commenced because he experienced flatus but had no defecation. Maintenance solution (43 g/L dextrose) and dextrose-free Ringer solution were administered at 40 mL/h. On POD 2, the patient consumed 80% to 100% of his diet, although defecation was not observed. The patient felt nauseous, and a flapping tremor was observed as his serum ammonia level increased to 187 µg/dL in the afternoon. Therefore, an intravenous infusion of a branched-chain amino acid (BCAA)-enriched preparation (Aminoleban®) (500 mL/day) was initiated at 150 mL/h.
Fig. 1
Serum ammonia levels and perioperative treatment. Serum ammonia levels ranged from 27 µg/dL to 46 µg/dL during anesthesia (a). Serum ammonia level increased to 894 µg/dL on POD 3 (b). Treatment included glycerin enema, intravenous glucose supplementation, cessation of protein intake, and control of defecation. Consequently, the serum ammonia level decreased to 165 µg/dL 1 h after defecation. The horizontal dotted line indicates a normal serum ammonia level (66 µg/dL). BCAA, branched-chain amino acids; POD, postoperative day
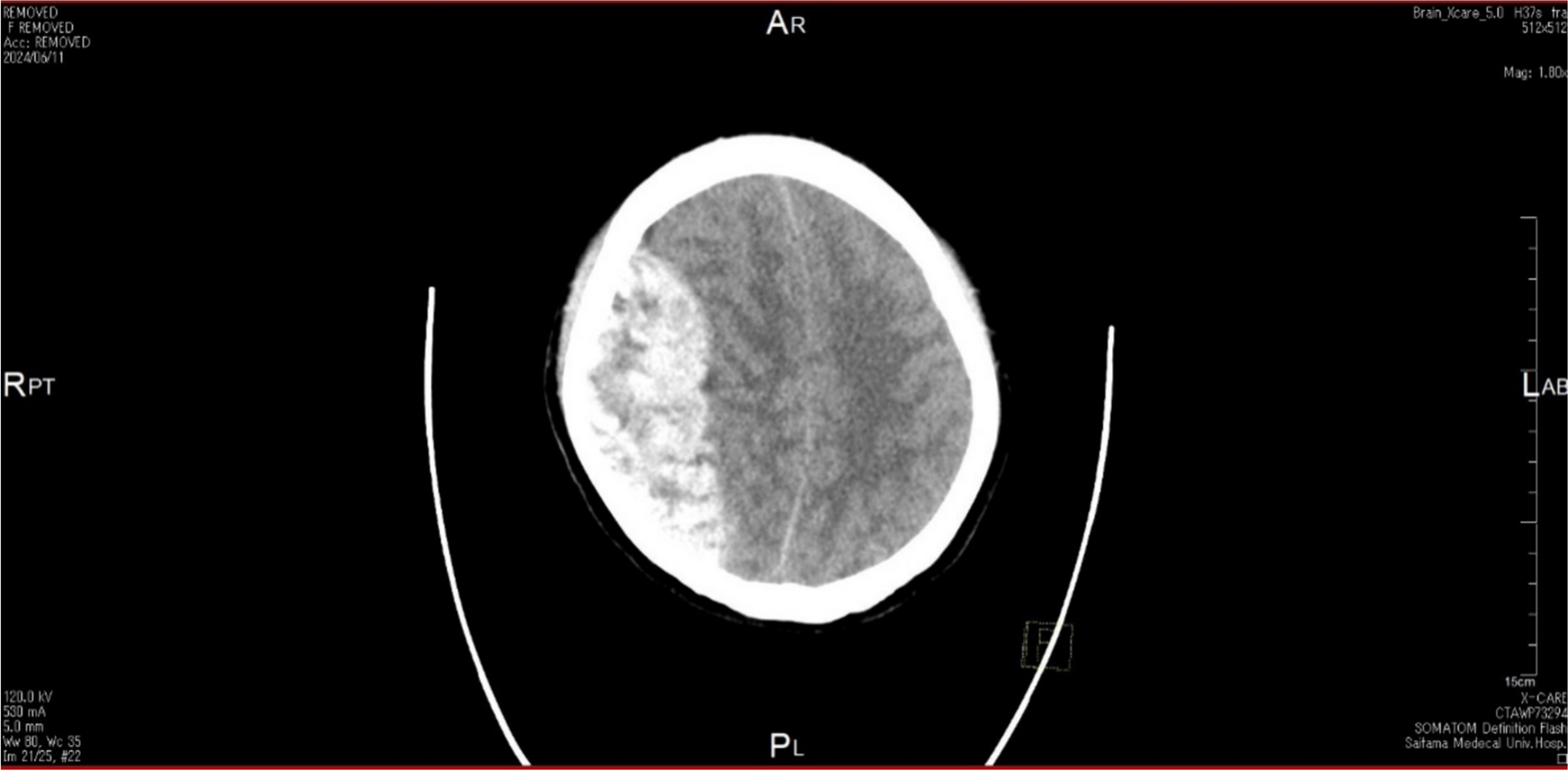
On the morning of POD 3, the patient was conscious; however, he was unable to eat due to worsening nausea. The diet was stopped, and dextrose-supplemented Ringer acetate solution (50 g/L dextrose) was administered. Intravenous infusion of a BCAA-enriched preparation (500 mL/day) was administered again in the afternoon. The patient vomited several times in the evening and became increasingly somnolent and agitated. The Glasgow Coma Scale (GCS) score was E3V2M5. Laboratory results showed an acute exacerbation of hyperammonemia (894 µg/dL). Arterial blood gas analysis on room air showed anion-gap metabolic acidosis and compensatory respiratory alkalosis. Computed tomography of the head showed no cerebral edema. The patient fell into a deep coma (GCS E2V3M2) and was admitted to the intensive care unit. The patient received intravenous hydration supplemented with dextrose and lipid emulsion. Furthermore, the patient received a glycerin enema and defecated. One hour after defecation, the serum ammonia level rapidly decreased to 165 µg/dL, and the state of consciousness improved (GCS E3V3M5). On POD 4, the patient remained somnolent. Therefore, the medication was resumed via a nasogastric tube. To control defecation, which was intentionally managed to induce diarrhea, magnesium oxide (1650 mg/day) and sodium picosulfate solutions were administered via a nasogastric tube. The serum ammonia level fluctuated between 97 and 220 µg/dL, depending on the defecation status. On POD 6, the serum ammonia level normalized, and his mental status improved (GCS E4V5M6). The patient was transferred to the general ward on POD 7, and defecation management and rehabilitation were continued. Subsequently, the patient’s clinical course was uneventful, and discharged on POD 45 without any complications.
留言 (0)