Aneurysm of Membranous Ventricular Septum is a less common form of septal disease [1]. According to scholars, AMVS accounts for 0.3% of all congenital heart diseases and 19.1% of VSD [2]. AMVS is formed in different periods from newborns to 6 years, but most often formed in the early stages of infancy [3]. Onat et al. [4] reported that spontaneous closure was strongly associated with AMVS formation, which is seen in 5% of adult patients.
AMVS is always a natural closure of the ventricular septal defect. VSD is subjected to high-pressure blood flow, resulting in endocardial fibroplasia around the VSD with irregular fibroplasia as well as adhesive fusion of the septal valve, the anterior septal valve junction, and some of the tendinous cords. Due to the hemodynamic changes, the morphology of the aneurysm is often altered.
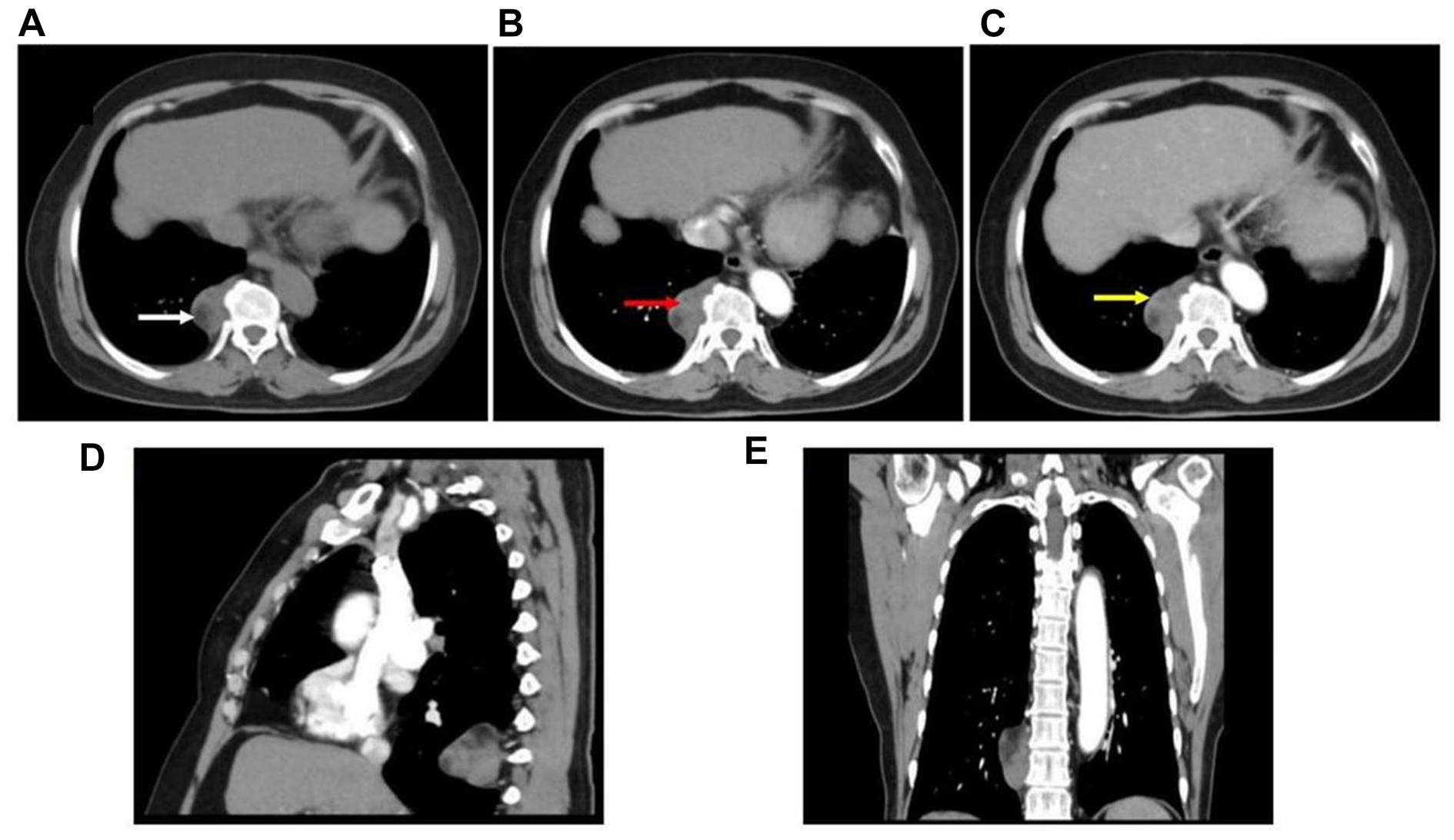
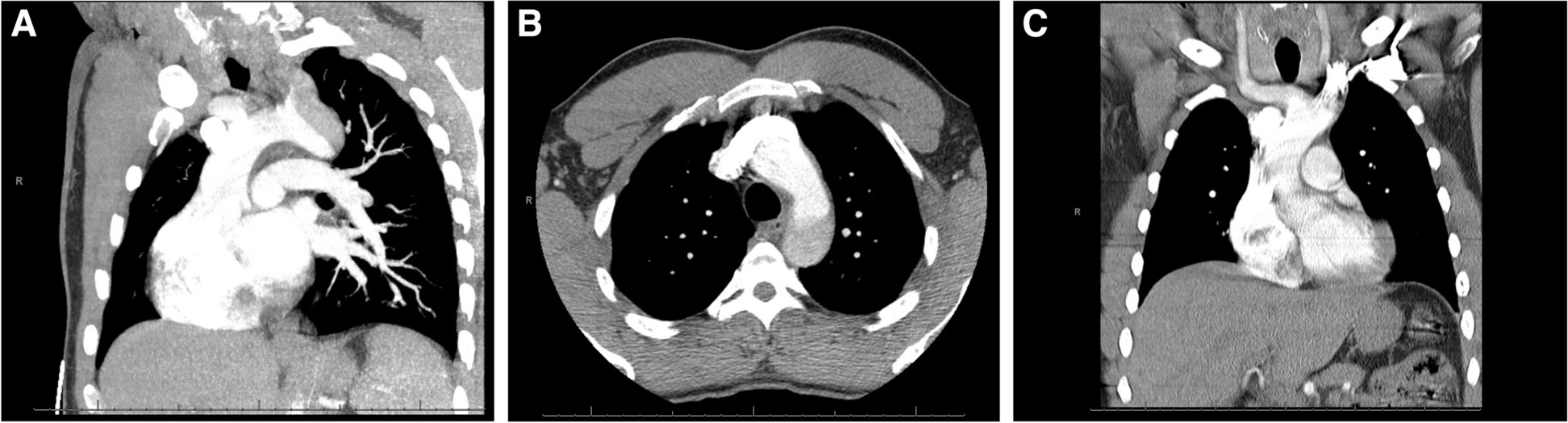
Aneurysms are usually reported as small to medium sized, ranging from 1 to 3 cm in diameter [5]. In this case, the diameter reached an astonishing size of 5 cm. The wall of the aneurysm was thickened irregularly due to the widespread calcification which may be related to prolonged blood flow impingement and an inflammatory response.
The membranous septum originates in part from the endocardial cushion and is close to the heart valves and conduction system. Therefore, the patient may experience ventricular block, which explains the abnormal ECG of the patient.
The main differential diagnosis of MVSD is aortic sinus aneurysm (ASA), also known as coronary sinus aneurysm. On TTE, the ASA is located above the aortic annulus, while the MVSD is located below the aortic annulus. In the present case, the aneurysm started below the aortic annulus, extended across it and ultimately grew along the aortic root. Both TTE and TEE showed no significant blood flow entering the aneurysm during systole, we hypothesized that this might be due to the widespread mural calcification of the wall. Commonly, biphasic flow exists in septal membranous aneurysm. However, in this case, due to the large size and widespread calcification of the aneurysm, the pressure gradient between the aneurysm and the left ventricle was not obvious, so there was no LV-AMVS shunt during systole. During the diastolic period, the pressure in the left ventricle decreased. At this time, there was a large amount of regurgitation of the aortic valve that should have been closed. These regurgitation from the aortic valve entered the aneurysm through the ventricular septal defect, formed eddy currents in the aneurysm, flowed into the left ventricle, and exited with the next cardiac cycle.
It has been shown that the incidence of aortic regurgitation and aortic valve prolapse is significantly higher in patients with AMVS (29% and 47%) than in patients with VSD (4.9% and 20.2%) [5]. Some scholars have reported the incidence of aortic regurgitation in unoperated pediatric or adult patients with VSD to be 5.5 – 18% [6]. Freedom and his colleagues reported aortic valve prolapse in 2 of 32 (6.25%) patients with AMVS [7]. The size of VSD may be an important factor contributing to aortic valve prolapse and regurgitation. A larger VSD can leave the aortic annulus unsupported, leading to secondary aortic annular dilatation.
In a series of studies by Yilmaz [5], AMVS was associated with serious complications. Aneurysm formation functionally reduces the size of the VSD, but has the potential to cause tricuspid valve insufficiency, aortic valve prolapse, right ventricular outflow tract obstruction, aneurysm rupture, and bacterial endocarditis.
In isolated membranous septal aneurysms without residual shunts, the defect diameter and index cross-sectional area of the aneurysm are predictive of prognosis, spontaneous closure and successful surgical closure [8]. Once the diagnosis of AMVS is confirmed, all surgical indications should be treated aggressively to avoid complications such as aneurysm rupture, obstruction, thromboembolism and endocarditis. With the increasing sophistication of surgical techniques such as interventional therapy, the prognosis of the disease is generally favorable.
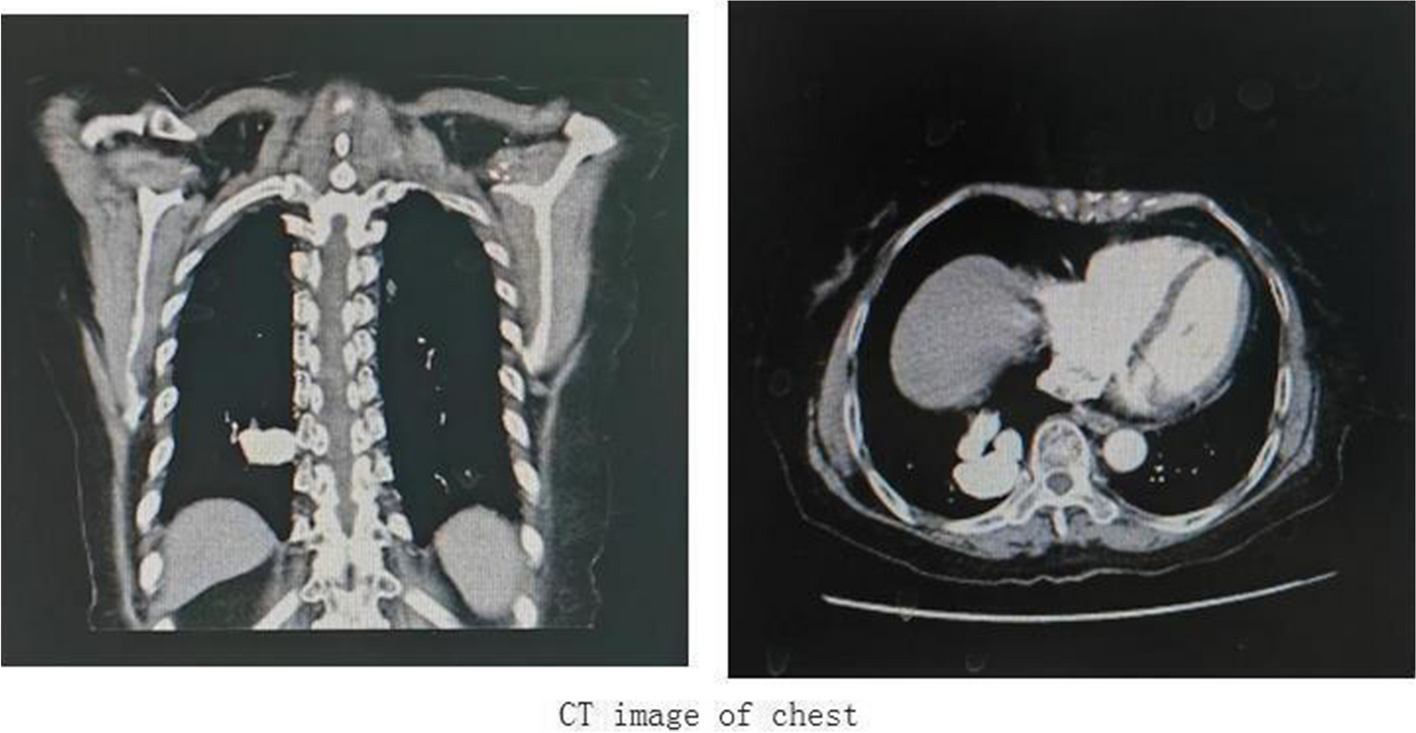
Coronary CTA is widely used in clinics because of its advantages of being non-invasive and simple [9]. It can clearly show not only the coronary artery but also the location of AMVS, the length and diameter of the aneurysm, the width of the basal portion, whether there is a thrombus in the aneurysm and whether the aneurysm is ruptured. Through multi-temporal reconstruction, the motion of the aneurysm can be observed dynamically, which provides clear and effective image data for clinical intervention in advance.
Echocardiography has a high clinical application value for AMVS. It can dynamically observe the changes of AMVS during each cardiac cycle. CDFI can display the blood flow signals and observe whether there is any blood flow entering AMVS. TTE or TEE should observe the position and size of the AMVS, as well as the relationship between AMVS and its surrounding structures.

留言 (0)