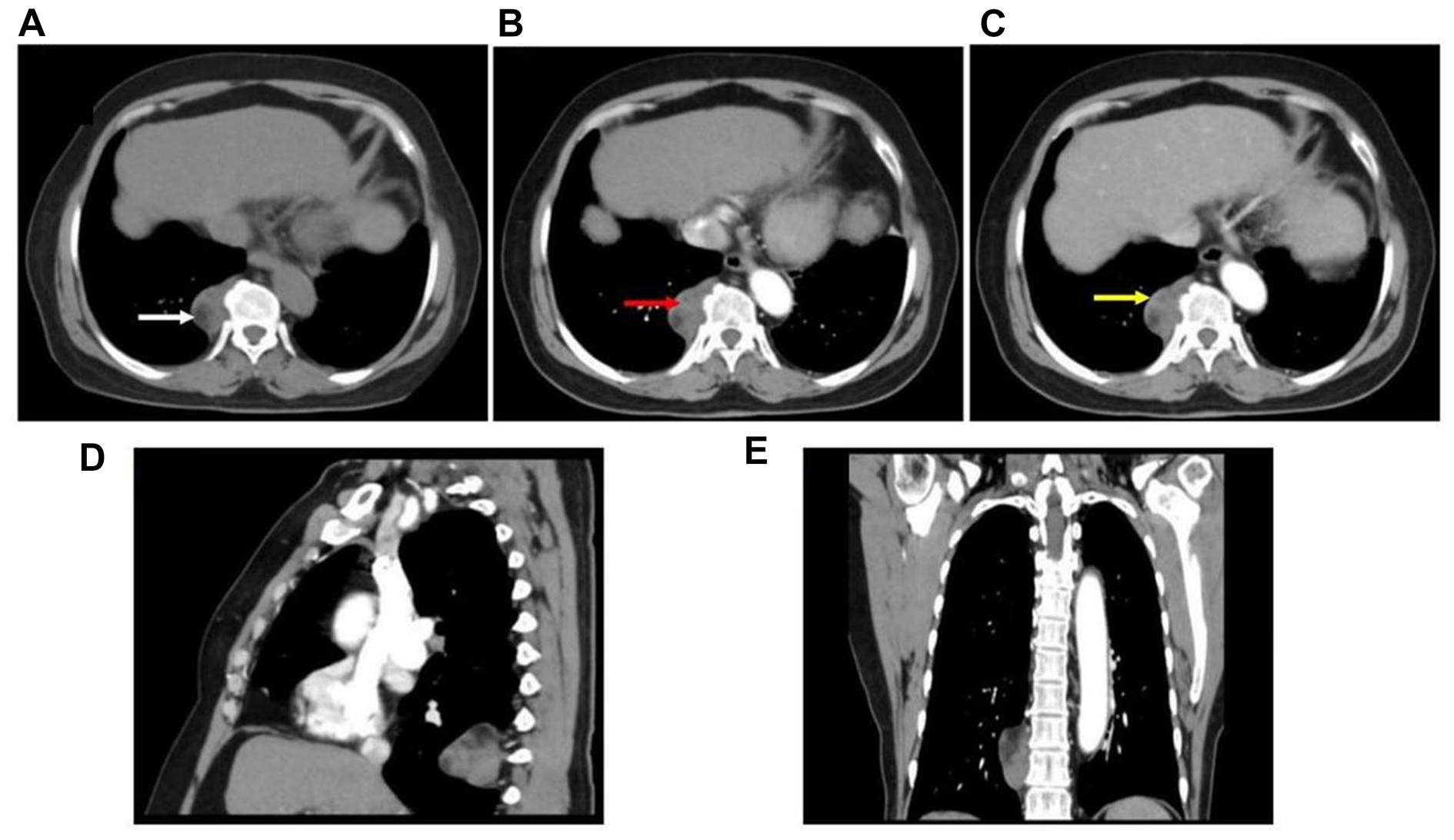
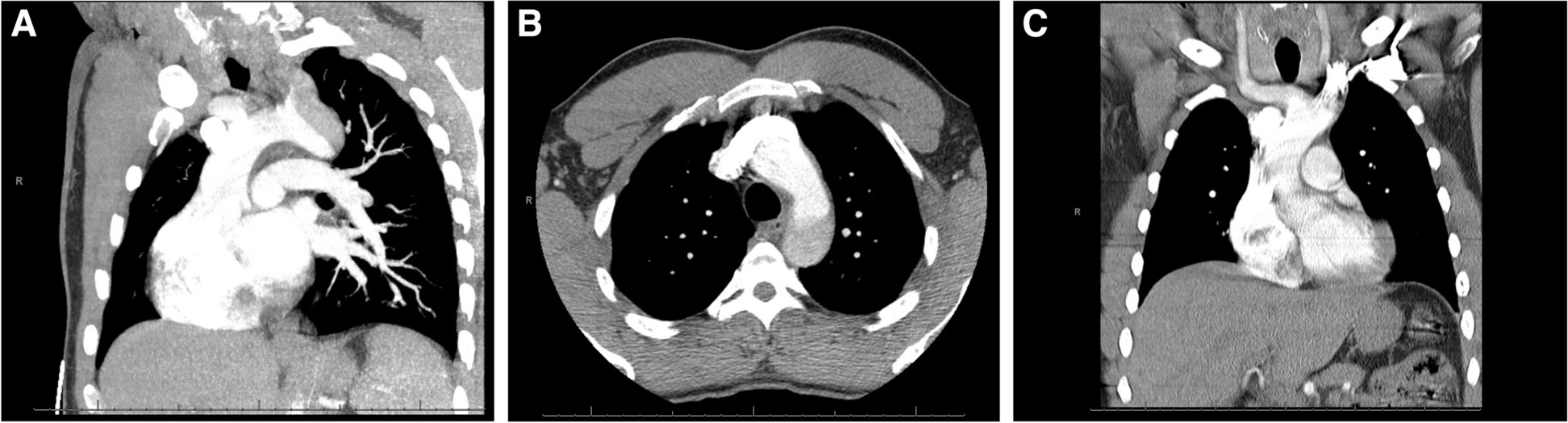
A shaggy aorta represent a category of critical importance that shows protruding eccentric plaques or thrombi on contrast-enhanced CTA finding and vulnerable aortic plaques and injuries on nonobstructive angioscopic and pathological findings. In particular, it is crucial to assess the perioperative atheroembolic risk caused by a shaggy aorta preoperatively. In view of the preoperative risk stratification, the severity of aortic arch atheroma was categorized according to the preoperative CT and TEE grades described by Gutsche et al. [1] and Katz et al. [2], respectively. The present patient was considered unfit for a total debranching TEVAR because he was diagnosed with severe grade V arch atheroma, which extends to the orifice of the innominate artery.
TAR-reinforcing brain protection is considered an effective treatment of choice for aortic arch pathologies associated with severe atheroma [3]. Furthermore, we observed strict adherence without touching the aorta until a deep hypothermic circulatory arrest was achieved. Reconstruction of the left CCA and left AxA at other incisions is a useful technique because it minimizes manipulation around the orifices of the neck vessels affected by severe atheromatous changes. Cerebrovascular events in TAR may occasionally occur because of debris embolization, which includes the non-physiological bloodstream of the extracorporal circulation, direct manipulation of the aorta and cervical vessels for cannulation or clamping, and incomplete brain protection. Furthermore, the presence of a shaggy aorta increases the risk for neurological complications [4].
Several methods for cerebral protection must be closely investigated while performing TAR. Although antegrade cerebral perfusion is widely used, it is impossible to prevent complete brain malperfusion due to incomplete intracranial vascular communication, heterogeneous perfusion of all three neck vessels, and an inadequate perfusion rate. In contrast, retrograde cerebral perfusion as a cerebral adjunct may have played an important role in preventing the dropping of plaque debris in the present case.
The brain isolation technique, which precedes and separates selective cerebral perfusion from systemic perfusion, may be a valuable adjunct for preventing cerebral embolization, as reported by Shiiya et al. [5] and Sawazaki et al. [6]; however, there is concern about the failure of brain perfusion at normal temperature, and it is not necessarily possible to clamp the neck vessels in patients with a shaggy aorta. In the present case, the functional brain isolation technique, which was composed of retrograde perfusion to the brain from neck vessels, except for left CCA, and unclamping of the orifices of neck vessels, was adopted as an effective alternative, although it was unclear whether adequate cerebral perfusion was ensured. Furthermore, it was possible that the fragile atheroma was unexpectedly stirred up to the left CCA with a turbulent jet, given that streamline analysis showed that the flow from both AxAs hit the lesser curvature of the aortic arch in the aortic arch aneurysm experimental model, as reported by Minakawa et al. [7]. This finding was sufficient to indicate the requirement for individual antegrade perfusion of the left CCA. In the present case, it was demonstrated that adding the left CCA to the bilateral AxAs as the arterial inflow for CPB could result in functional total occlusion in the native left CCA,as evidenced by individual measurements of the perfusion flow rate.
The frozen elephant trunk (FET) technique, which takes advantage of endovascular technology, has been introduced as a single-stage procedure for TAR. Even if a severe atheroma inside the aorta is visible directly under deep hypothermic circulatory arrest, a stent graft introduced by antegrade delivery, that is, the FET, may scratch and scatter a rugged shaggy arch aorta blindly and carry a high risk of debris embolization. In the present case involving CET, it is crucial to meticulously select and insert the tube graft according to the length of the aneurysm, while minimizing contact with the inner surface of the aneurysm as much as possible. The incidence of new distal stent graft-induced entries following the FET technique is reportedly higher than that following conventional TEVAR [8]. Spinal cord injury in patients undergoing FET was reported to be significantly higher than that in patients undergoing CET [9]. Spinal cord injury after TEVAR in patients with prior infrarenal AAA repair occurs significantly compared with that in patients without prior AAA surgery, as reported by Schlösser et al. [10]. In this patient with prior infrarenal AAA repair, it was crucial to pay attention to avoid intraoperative hypotension during TEVAR. There is concern that simultaneous and parallel TAR and TEVAR may cause progressive intraoperative hemodynamic instability associated with hypotension due to bleeding. Furthermore, anastomosis to the descending thoracic aorta distal to the aneurysm, requiring thoracotomy, appeared to be an invasive surgical option, particularly in the present case of comorbidities. Therefore, TAR with CET in combination with secondary TEVAR was considered to be the appropriate treatment of choice.
Patients with a shaggy aorta may potentially benefit most from the two-step approach, in which a conventional stent graft is secondarily placed in the intended place within the CET retrogradely while providing a sufficient proximal landing zone. Secondary conventional stent graft implantation supports precise deployment of the stent graft to its intended position, completely excluding the diseased aortic segment, under prudent TEE and fluoroscopic guidance. Skillful manipulation of guidewires, catheters, and devices during endovascular therapy is important to protect against embolization to the abdominal viscera and lower extremities. Neither an adjunctive technique to prevent embolization to the abdominal viscera and lower extremities nor cerebrospinal fluid drainage to reduce spinal cord injury was used in the present case. Therefore, it is crucial to consider the merits and demerits of these approaches on a patient-to-patient basis.
Additionally, TEE would surely contribute to the evaluation of severe atheroma plaques, including mobile components, as a sensitive modality and to the precise deployment of the stent graft in a nondiseased descending aorta.
In summary, our integrated treatment strategy for TAR in patients with a shaggy aorta can be described as follows: the condition of being far from the atherosclerotic burden in the arterial inflow for CPB, the functional brain isolation technique, no touching of the atherosclerotic aorta until the deep hypothermic circulatory arrest is achieved, retrograde brain perfusion to prevent the dropping of debris, conversion to antegrade brain perfusion as soon as possible after an arch-first approach, and the CET technique as a useful adjunct to TAR to provide an excellent proximal landing zone for prospective stent graft implantation in the downstream aorta. The present case suggests that TAR with CET and secondary thoracic endovascular aortic repair may be an effective alternative for aortic arch pathology with a shaggy aorta. Nevertheless, the strategy for surgical treatment in patients with aortic arch pathologies and a shaggy aorta must be judged on a case-by-case basis.

留言 (0)