We performed sex- and gender-disaggregated analyses of AE survey data for two different mandated vaccines—the quadrivalent influenza and bivalent COVID-19 vaccine—to examine vaccine outcomes and vaccine-related behaviors among a cohort of adult HCWs, which can inform public and occupational health vaccine strategies and policies.
In our study population, influenza and COVID-19 vaccines do not cause serious AEs with localized, mild AEs being the most common experience [34, 35]. The bivalent COVID-19 vaccine recipients reported higher rates of AEs compared to influenza vaccine recipients in our cohorts, consistent with a retrospective analysis of VAERS data [36]. Increased AE reporting rates among COVID-19 vaccine recipients may be potentially confounded by the heightened scrutiny and vaccine hesitancy against mRNA COVID-19 vaccines at the time but is still important to note for public health and education purposes. While the term “adverse event” may suggest harmful or negative effects, non-serious AEs are normal and healthy manifestations of the immune system’s response to the vaccine antigen [10]. Transparent and consistent reporting of AEs is imperative to normalize these vaccine-related experiences, mitigate fear and misinformation, and encourage vaccine uptake.
Studies identifying age effects on the reporting of AEs are most common among older aged vaccinees (i.e., 65 years and older). Among adults 75 years and older, females have a greater probability of reporting any AE, either local or systemic, which significantly decreases with increasing age for females, but not for males, after influenza vaccination [2]. Further, the proportion of COVID-19 vaccine AEs is greatest among younger adults (i.e., 18–64 years of age) while the proportion of serious AEs is greatest among older adults (i.e., 65 years and older) [37]. Our analyses did not identify a significant age effect on the reporting of AEs following influenza or COVID-19 bivalent vaccination, likely because the cohort was predominately younger and reproductive-aged individuals, a population that has not been previously evaluated in the context of AEs following vaccination.
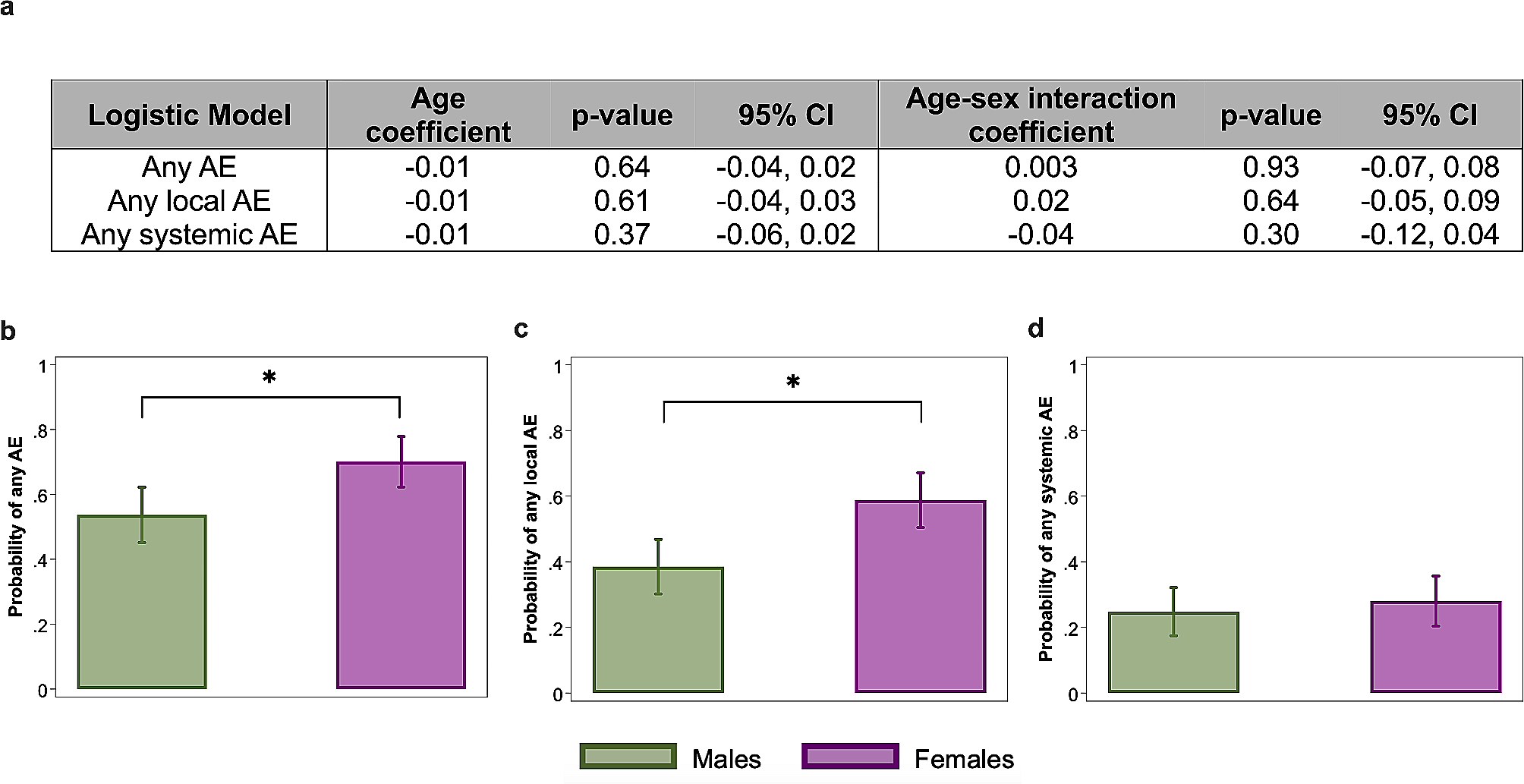
Sex-disaggregated analyses reveal that female HCWs were significantly more likely to report local AEs, but not systemic AEs, after receipt of either the influenza vaccine or bivalent COVID-19 vaccine. Similarly, an active surveillance study of predominately younger adults (i.e., 20–49 years of age) in South Korea reported females having significantly more AEs, local or systemic, after receiving the first dose of ChAdOx1 nCoV-19 (AstraZeneca/Oxford) vaccine as compared to males based on self-reported survey results at 3 days post-vaccination [38]. In another highly vaccinated population of older adults (75+), females had greater probabilities of reporting local AEs, but not systemic AE, compared to males after receipt of the high-dose quadrivalent influenza vaccine as measured by AE surveys [2]. Real-world data extracted from the Vaccine Adverse Event Reporting System (VAERS) highlight that although more adult (i.e., 18–64 years of age) females reported AEs within one week of COVID-19 vaccination, males have 1.5 times greater odds of reporting serious AEs [37].
Further disaggregation by sex and self-reported race demonstrates that females, regardless of race, consistently have a higher probability of experiencing local AEs with sex comparisons of White or Black participants reaching statistical significance. The probability of experiencing a systemic AE was comparable between sexes, regardless of race. While we did not find differences among racial categories, consideration for race and ethnicity analyses are important for vaccine studies. Race is not a biological variable associated with AEs, but race and ethnicity have been widely reported as important predictors of vaccine behaviors and perceptions [1, 39,40,41,42]. In a survey study of over 10,000 HCWs, COVID-19 vaccine hesitancy is highest among Black and Hispanic or Latino HCWs when compared to White HCWs with concerns about side effects being the most frequently cited reason [39].
Sex differences in adverse events are not specific to vaccines and have also been reported for other therapies, such as cancer immunotherapies, suggesting an underlying biological mechanism [43,44,45]. In a study of small-cell lung cancer patients receiving chemotherapy, although a greater proportion of females have more chemotherapy toxicity (e.g., hematologic toxicity, stomatitis, and vomiting) than males, females also have higher response rates and longer median survival times than males [44]. A meta-analysis of 202 clinical trials of cytotoxic therapy, immunotherapy, and targeted therapies [38] reported that females have significantly greater odds of severe toxicity and a 66% increased risk of symptomatic AEs compared to males. Unlike vaccines that are mass-produced, personalized medicine may provide new avenues for other therapies or drugs, especially those with more severe AEs, to address sex differences in AEs [46].
The female-bias in AEs has been documented for COVID-19 and influenza vaccination [2, 3, 17, 47, 48], yet the role of sex steroid hormones in the manifestation of vaccine AEs for either males or females is not clearly understood. Although our study was not designed to evaluate the hormonal and immunological responses associated with post-vaccination AEs, we used hormonal birth control data (e.g., contraceptive use, IUD, implant, etc.) among females as a surrogate to assess if exogenous hormones were associated with reporting of AEs. Our data revealed that reporting of AEs did not differ by hormonal birth control use among young, reproductive-aged female HCWs. This may be due to reproductive-aged females already having sufficient endogenous sex steroid hormones such that birth control (i.e., exogenous hormones) did not change the experiences of vaccine AEs. Whether exogenous hormone use among postmenopausal women affects the experiences of vaccine AEs requires consideration.
While more studies are implementing sex-disaggregated analyses, gender-disaggregated analyses are sparse in biomedical research due to the lack of an objective, standardized methodology for measuring gender and persistent misunderstanding of how to define gender and sex. Examining vaccine outcomes and behaviors with a gender lens (i.e., consideration of how social or cultural norms impact behavior) can inform public health messaging strategies and improve vaccine uptake. For instance, studies have found women have greater influenza and COVID-19 vaccine hesitancy compared to men worldwide [22, 23, 40, 49,50,51]. A survey of HCWs in New York found that men had a higher likelihood of planning to get the COVID-19 vaccine within the next six months than women [27]. Although pregnancy and breastfeeding have been hypothesized as factors contributing to reduced vaccine uptake among women, a previous study found no differences in vaccination uptake between reproductive-aged and non-reproductive-aged women [27]. HCWs are a unique population with increased access to accurate vaccine and medical information, yet vaccine hesitancy, particularly due to AEs, persists even when vaccines are mandatory because of occupational exposure and spread [25, 26, 28].
Gender differences in vaccine behaviors pertaining to AEs are understudied. To our knowledge, we are among the first to integrate qualitative measures through open-ended survey questions to provide insight and context for differences in vaccine AE perceptions among men and women. Our qualitative thematic analysis of open-ended answers revealed that, by proportion, more women mentioned seeking out self-treatment (e.g., over-the-counter pain medications) for their AEs and to experience disruptions in their daily routines than men after bivalent COVID-19 vaccination. Compared to men, women mentioned that AEs affected their ability to take care of their families, which is likely related to the gender norms and roles around caregiving in the United States [52]. In the meta-analysis [8], more women than men reported experiencing moderate to severe levels of inconvenience after influenza vaccination. In our study, experience of AEs from prior vaccinations motivated some women, but not men, to schedule their COVID-19 vaccinations on a day prior to their scheduled time off. Further interrogation of these gender differences in vaccine AE-related behaviors may inform vaccine campaign strategies or messaging, particularly among working-aged populations who are mandated to take vaccines due to occupational exposure or spread.
According to the 2019 U.S. Census Bureau women comprised 76% of healthcare jobs with 85% of nursing and health aide positions held by women [32]. We found that women HCWs were more likely to experience AEs than men and were more likely to seek out self-treatment and/or schedule vaccination prior to their days off from work. In a California survey of over 2,000 HCWs studying COVID-19 vaccine side effects, 28% experienced side effects that were disruptive to work and 18% missed work [53]. The authors also found that 6.7% of physicians missed work as compared to 21.2% of other HCW roles. Presenteeism, working despite feeling unwell or sick, and absenteeism are linked to occupational expectations and pressures that may differ across HCW roles, and can impact the quality of patient care, occupational burnout, and employee morale [53]. With nearly 9 million HCWs nationwide receiving mandated vaccinations, we can expect that millions of workers will experience AEs annually with potential occupational health and labor force implications, including increased vaccine hesitancy, missed work, and disruptions to recognized time off, that may disproportionately affect women. Our data add gender to the list of factors that need to be considered in policies surrounding mandatory vaccines, including, for example, receipt of paid medical leave.
Limitations
There are several limitations to this study. First, the enrollment criteria (e.g., limited age range) were different and did not allow for deeper interrogation into the effects of longitudinal age-related differences in our two cohorts. The sample size of males and females enrolled were only pre-specified and balanced for the influenza vaccine cohort (n = 50 females and 50 males per season) and not the bivalent COVID-19 vaccine cohort (n = 150 females and 46 males); therefore, the COVID-19 vaccine cohort may be more representative of the HCW demographics. Highly vaccinated HCWs are more likely to be biased towards vaccine acceptance and the interpretations made from this unique demographic may not be applicable to non-HCW populations. Second, the criteria and definitions for local and systemic AEs used may differ from other studies. AEs were surveyed two days post-vaccination, so we were unable to assess AEs after administration of the questionnaires. Third, we did not conduct in-depth interviews nor balance sample sizes for the gender difference analyses. Open-ended survey responses were used for the thematic analysis of vaccine-related behaviors and predominately consisted of responses from women, due to the demographics and study design for the COVID-19 vaccine cohort. Lastly, biological samples were not collected from participants; therefore, we were unable to study the immunological mechanisms by which sex causes differences in AEs.



留言 (0)