Study design and creating study groups
This is a prospective study conducted on girls with premature thelarche and age-matched healthy prepubertal controls. The study included all girls referred to the pediatric endocrinology outpatient clinic between June 2021 and February 2022 due to breast development before the age of 8 years.
Once premature thelarche was confirmed by a pediatric endocrinologist, these girls underwent a series of investigations, including physical examination, biochemical tests, hand and wrist X-ray, pelvic ultrasound and luteinizing hormone-releasing hormone (LHRH) stimulation test to distinguish between ICPP and isolated premature thelarche (IPT). Girls diagnosed with precocious puberty underwent contrast-enhanced brain and pituitary MRI. Those found to have an organic pathology were excluded from the study, leaving only idiopathic cases.
After forming the patient groups, prepubertal healthy controls of similar ages to the patients were recruited from the general pediatric outpatient clinic. These controls included children who presented for a routine check-up or with concerns about height, weight, or pubertal development and were ultimately found to be free of any endocrinological disorders. Inclusion criteria for the controls included not having a chronic disease, not taking medication, and being at Tanner stage 1 based on the examination by a pediatric endocrinologist. Finally, three groups were formed: the girls with ICPP, the girls with IPT and prepubertal controls.
Evaluation of the subjects
All girls underwent anthropometric measurements, including height and weight, using a stadiometer (Holtain Limited, Crymych, Wales) and an electronic scale (Tanita MC-780 MA, Tanita Corporation, Tokyo, Japan). Standard deviation scores (SDSs) for height, weight, and BMI were calculated according to the standards for Turkish children [16]. Pubertal stage was assessed based on the Tanner scale [17].
Girls with premature thelarche underwent initial biochemical tests, including serum follicle stimulating hormone (FSH), LH, estradiol, thyroid-stimulating hormone (TSH), and free thyroxine (fT4). Bone age was determined using the Greulich and Pyle method. A GnRH stimulation test was performed with a standard dose of 0.1 µg GnRH administered as an intravenous bolus. Blood samples for FSH and LH were collected just before the injection and at 30 min intervals until the 120th minute after the injection. A peak LH value of more than 5 IU/L was considered suggestive of puberty. In pelvic ultrasound, a uterine length of more than 35 mm and ovarian volumes above 2 cc were considered consistent with puberty [18].
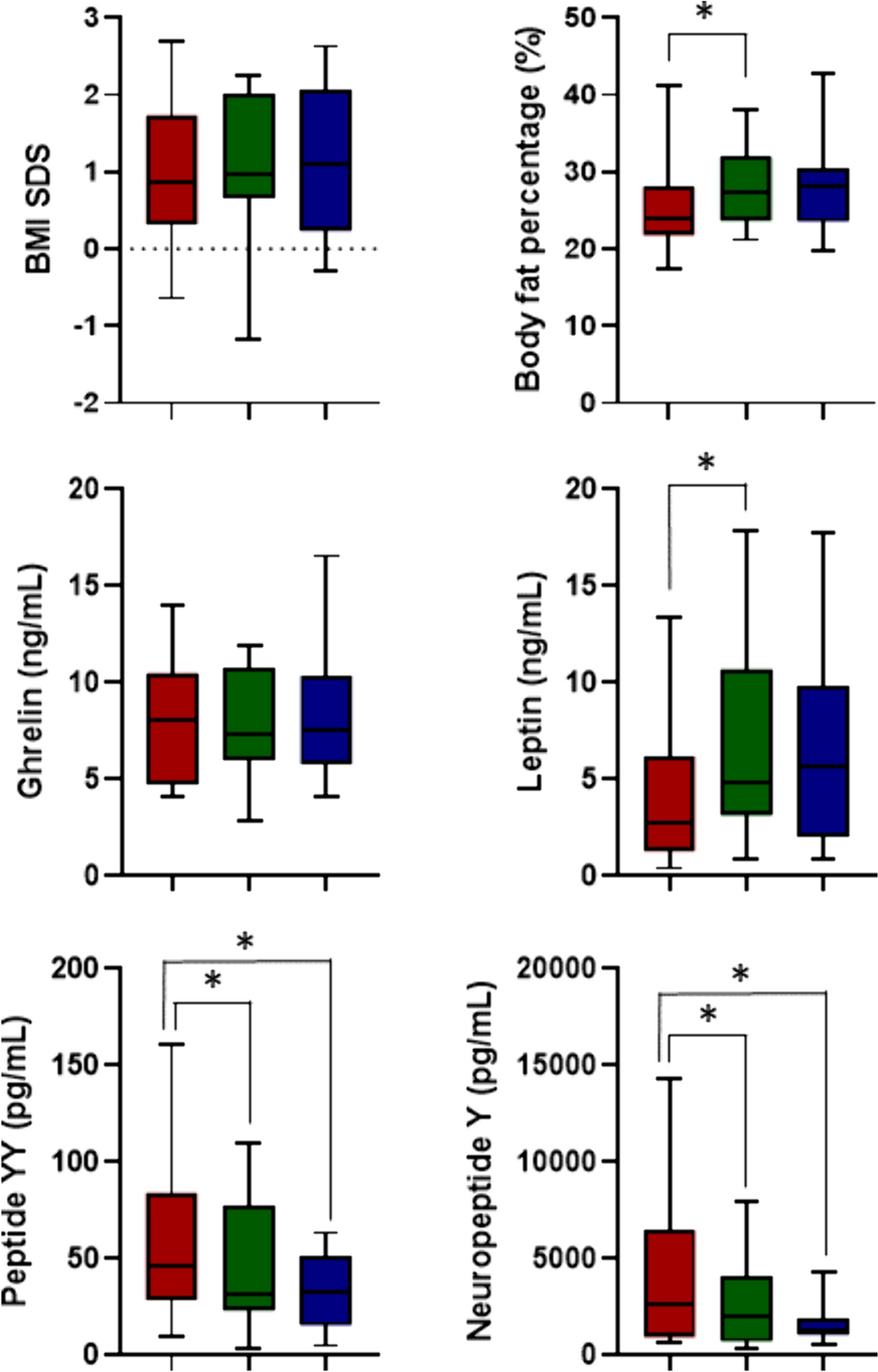
Body composition analysis was conducted using the bioelectrical impedance method (Tanita MC-780 MA, Tanita Corporation, Tokyo, Japan). A dietitian obtained a 24 h dietary recall, and total caloric intake, carbohydrate, fat, and protein intake, as well as macronutrient ratios, were calculated using Ebispro for Windows (BeBiS v.9) (Stuttgart, Germany).
Biochemical analysis
Blood samples were collected after an overnight fasting state, centrifuged, and stored at -80 °C until analysis for measurements of ghrelin, leptin, PYY, and NPY levels. The measurements were carried out using enzyme-linked immunoassay (ELISA) kits (Elabscience Biotechnology Co., Ltd, China for ghrelin, PYY, and NPY; DRG International, Inc., USA for leptin) with an absorbance microplate reader (BioTek ELx800, USA) following the manufacturer’s instructions. FSH, LH and estradiol levels were measured by electrochemiluminescence immunoassay (ECLIA).
Treatment protocol and monitoring of the patients with precocious puberty
Girls diagnosed with ICPP were initiated on leuprolide acetate treatment. The patients were prescribed either 3.75 mg of leuprolide acetate every 28 days (Lucrin Depot® 3.75 mg, AbbVie, Tokyo, Japan) or 11.25 mg every 3 months (Lucrin Depot® 11.25 mg, AbbVie, Tokyo, Japan). The treatment approach followed a predetermined sequential method, with patients alternating between the two dosage options. After starting treatment, clinical evaluation, body composition analysis, blood sample collection for measuring appetite-regulating hormones, and a 24 h food intake record were repeated at the 6th and 12th months. Additionally, serum LH levels were measured 30 and 60 min after leuprolide acetate injection at these milestones. Pubertal suppression was defined as a stimulated LH level less than 4 IU/L [19].
Statistical analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS), version 27 (Chicago, Illinois). Data distribution was evaluated through histograms and the Shapiro–Wilk test. Data with a parametric distribution were presented as mean ± SDS, while data with a nonparametric distribution were presented as median (minimum–maximum). Comparisons among the three groups were conducted using either the Kruskal–Wallis test or one-way analysis of variance (ANOVA), depending on the data distribution. Parameters within the ICPP group at 0, 6, and 12 months of treatment were compared using either repeated measures ANOVA or the Friedman test, depending on the data distribution. In cases where the Friedman test yielded statistical significance, post-hoc tests were conducted using the Wilcoxon signed-rank test with Bonferroni correction for pairwise comparisons. A Spearman correlation analysis was employed to assess the relationships between non-normally distributed variables. A p-value less than 0.05 was considered statistically significant.
Ethical considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Istanbul University-Cerrahpaşa. Informed written consent was obtained from the parents of all subjects to participate in the study.



留言 (0)