
記住我
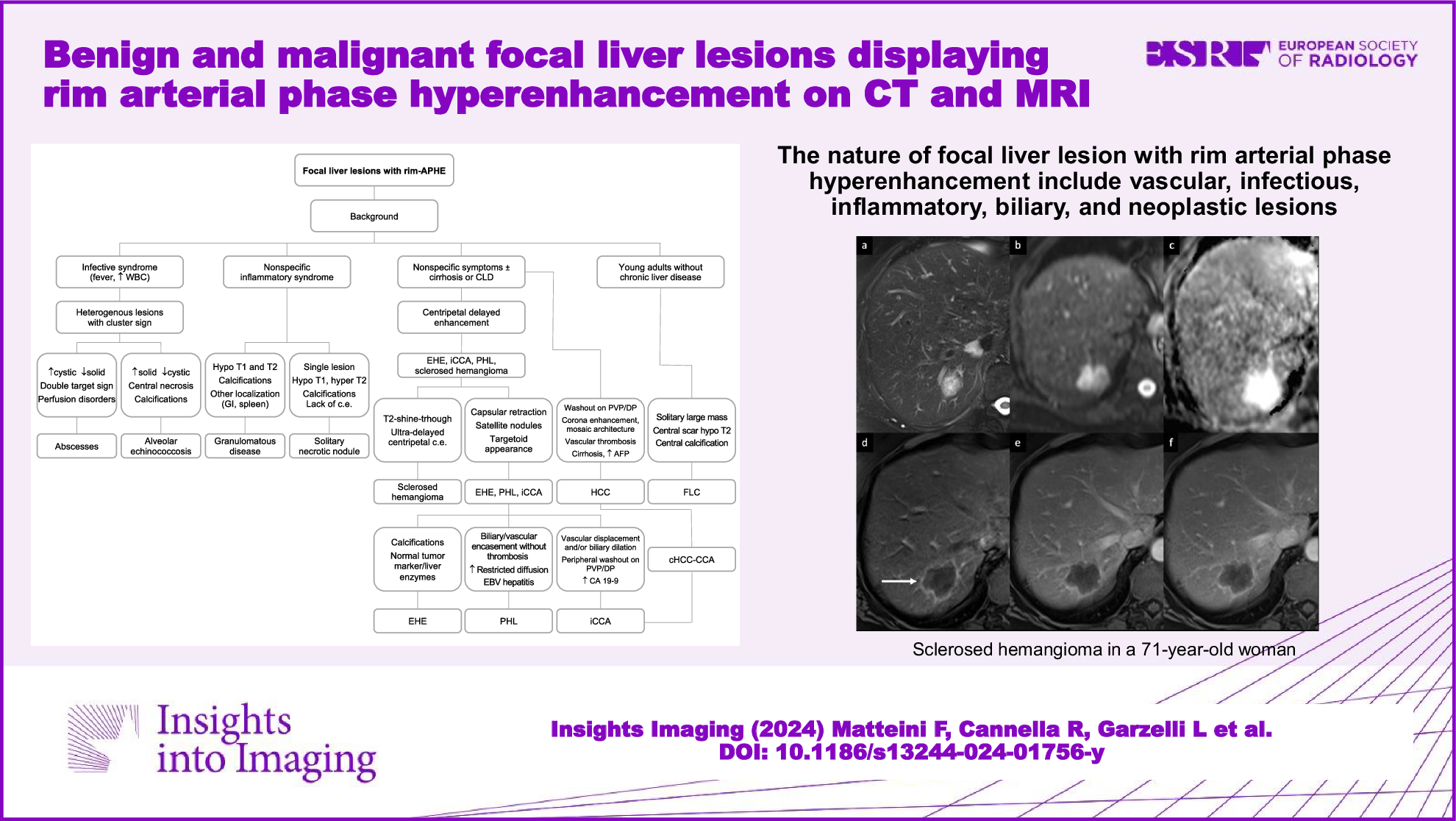



This single-center prospective study was approved by the Institutional Review Board of the National Cancer Center/Cancer Hospital, Beijing, China (No. 20/412-2608). The written informed consent was obtained from all participants. Between January 2020 and December 2021, consecutive patients underwent MR imaging examinations with quantitative DCE sequence due to suspected malignant hepatic lesions. The inclusion criteria were as follows: (1) over 18 years without other malignancies; (2) BCLC stage A: solitary HCC > 2.0 cm, no obvious macrovascular invasion or extrahepatic spread; (3) no anti-tumor therapeutic intervention. A total of 223 patients met the above criteria initially. 90 patients were excluded due to various reasons (Fig. 1). Finally, 133 patients including 112 men and 21 women with a median age of 57 years (range, 30–73) were included in this study. In order to build the prediction nomogram for MVI, the patients were randomly divided into a training set (n = 93) and a validation set (n = 40) at a ratio of 7:3 using a random seed method. The flowchart of the study population selection is displayed in Fig. 1.
Fig. 1
Flowchart of the recruitment of the study population. DCE, dynamic contrast enhanced; iCCA, intrahepatic cholangiocarcinoma; HCC, hepatocellular carcinoma; PEComa, perivascular epithelioid cells tumor; FNH, focal nodular hyperplasia; MVI, microvascular invasion
MR imaging acquisitionAll MR imaging studies were performed with a 3.0-T scanner (SIGNATM Architect, GE Healthcare, USA) equipped with a 46-channel adaptive image receive body coil. The magnetic resonance imaging (MRI) scan protocols and detailed acquisition parameters of the MRI sequences used are presented in Appendix E1 and Supplementary Table S1. Quantitative DCE-MRI was performed by using liver acquisition with volume acceleration-extended volume sequence according to our previous study [24]. In short, a multiple flip angle method ranging from 3° to 12° was adopted for T1 mapping which was used for the determination of tissue baseline T1 values, and a dynamic enhanced scan with 42 consecutive phases was performed for perfusion quantification.
DCE MR image processing and analysisThe DCE-MRI was processed using an in-house program written on MATLAB R2018a (MathWorks, Natick, MA, USA). The detailed image post-processing method is described in Appendix E2. The following six pseudo-color maps of the hemodynamic parameters were generated by a voxel-based curve fitting method using all DCE images as input: arterial fraction (ART, %), arterial flow (Fa, mL/min/100 g), portal-venous flow (Fp, mL/min/100 g), total blood flow (Ft, mL/min/100 g), distribution volume (DV, %), and mean transit time (MTT, s).
DCE MR images were analyzed by two independent radiologists (Y.J.Z. with 12 and W.C. with 6 years of experience in abdominal imaging) who were blinded to clinical, pathological, and laboratory information. Freehand-based region of interest (ROI) was manually segmented on the portal-venous phase DCE images using dedicated software (3D Slicer version 5.2.2; https://www.slicer.org/). The intra-tumoral ROI was carefully delineated along the contour of the tumor by referring to T2WI and DWI. Based on a topological algorithm from the tumor margin, the peritumoral ROI was automatically dilated at a radius of 10 mm, and manual correction was performed when the dilated ROI extended beyond the liver boundary. The ROIs were simultaneously copied to DCE perfusion maps and the mean values of DCE parameters in ITR (Fa-T, Fp-T, Ft-T, ART-T, DV-T, and MTT-T) and PTR (Fa-P, Fp-P, Ft-P, ART-P, DV-P, and MTT-P) were automatically extracted. The average measurements from two radiologists were used for the final analysis.
Conventional MR imaging featuresAll MR images were reviewed by two board-certified radiologists (S.W. and B.F., with 20 and 10 years of abdominal radiology experience, respectively), who were blinded to the patients’ clinical history and pathological information. Fourteen LI-RADS v2018 imaging features [25] and four non-LI-RADS imaging features (cirrhosis, tumor margin, tumor capsule, and two-trait predictor of venous invasion (TTPVI)) were analyzed. Any discrepancies were settled by consulting a third senior professor (X.H.M., with over 25 years of experience in abdominal imaging), and consensus was reached after discussion. TTPVI was defined as the presence of “internal arteries” in the arterial phase and the absence of continuous “hypodense halos” in the portal-venous or delayed phase [26, 27]. The definitions of each MR imaging feature are described in Supplementary Table S2.
Clinical characteristics, surgery, and pathological examinationThe baseline clinical characteristics were collected from the electronic medical records. All patients underwent AR or NAR radical hepatectomy as appropriate, which was determined by a multidisciplinary team discussion. The MVI status, degree of differentiation, histologic pattern, and fibrosis stage were evaluated and recorded on postoperative specimens.
Follow-up and endpointsPatients were followed up regularly at the outpatient clinic every 3 months within 2 years after hepatectomy and every 6 months thereafter, based on AFP and imaging examinations. The study endpoint was recurrence-free survival (RFS). Tumor recurrence was diagnosed according to the criteria of the EASL Clinical Practice Guidelines [17]. The RFS time was defined as the time interval from surgery to the first date of tumor recurrence or the last follow-up before December 31, 2023.
Statistical analysis and model constructionVariables were compared using independent sample t-test, Mann–Whitney U-test, χ2, or Fisher exact test as appropriate. Interobserver variability was assessed by the intraclass correlation coefficient (ICC) or Cohen’s kappa coefficients (κ-values) [28]. Multivariate logistic regression was used to identify independent predictors and construct the prediction models. A combined DCE parameter (CDCE) was generated based on the linear predictors of the regression equation (the sum of the intercept and independent DCE parameters multiplies the regression coefficients). A visualized combined nomogram was established using independent CR features and CDCE. Finally, the validation set was used to assess the model generalization. The receiving operating curve (ROC) was used to evaluate the predictive performance. Delong test was adopted to compare the predictive performance of ROCs among the models. The Hosmer-Lemeshow goodness-of-fit test and calibration curve were used to evaluate the model’s calibration. Decision curve analysis (DCA) was used to evaluate the clinical value of the combined model. Survival curves of different risk groups and surgical approaches were calculated by the Kaplan–Meier method and compared by log-rank test. A two-tailed p < 0.05 was considered statistically significant. All statistical analysis was performed using R software (version 4.2.2; R Foundation, Vienna, Austria).
留言 (0)