
記住我
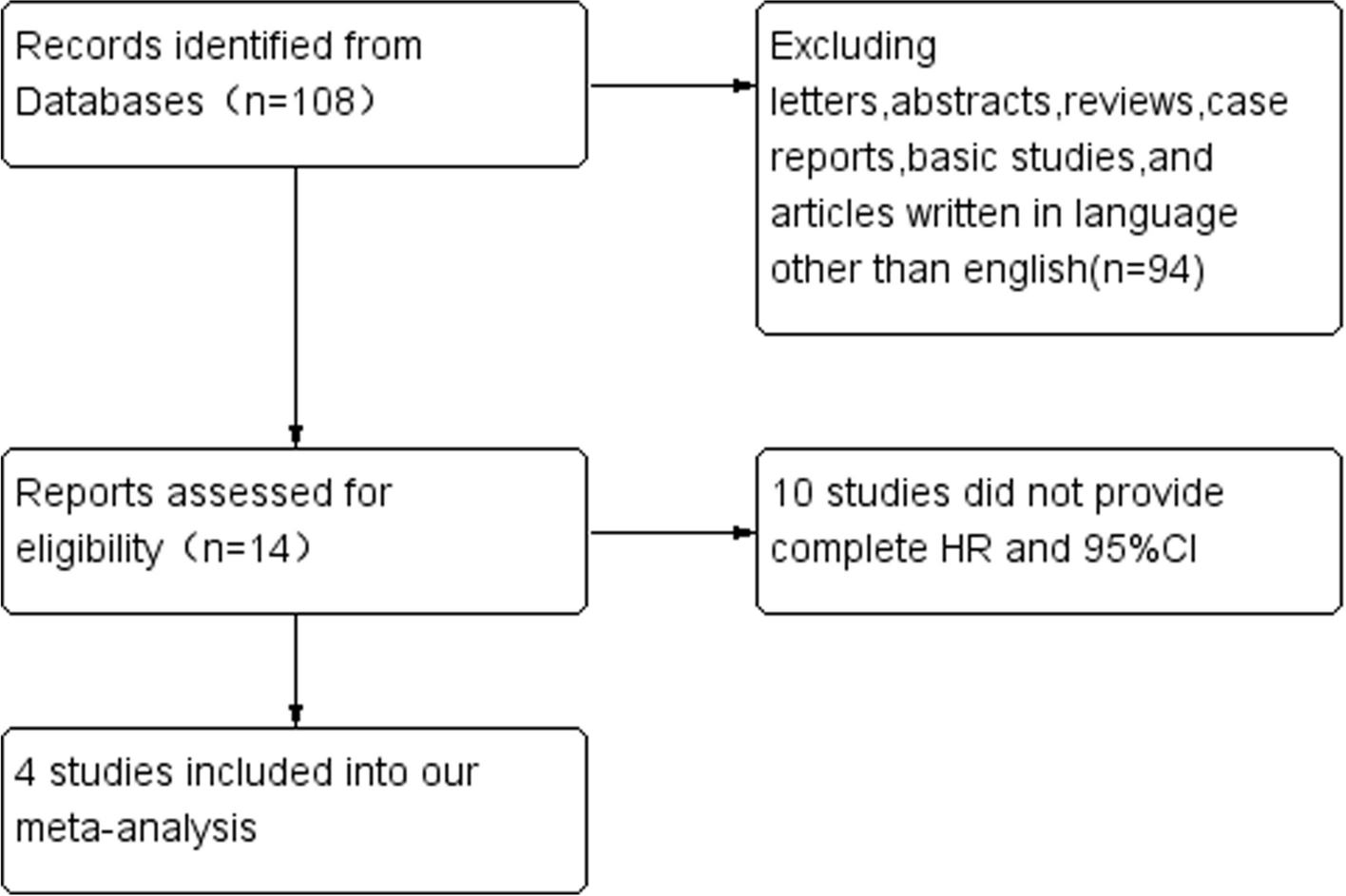
The initial research yielded 265 potential articles, after reading the titles and abstracts,245 studies were excluded because they were obviously irrelevant to our study design. The remaining 20 studies with full texts were carefully assessed for eligibility. As a results, 10 studies were excluded for following reasons: six studies did not provided the sufficient information for us to extract the data, one study choose hydrogel plug as control, two studies were non-comparative studies, one study was conducted in animal. At last 10 studies with 3874 patients (1904 in ABP group and 1970 in control group) [7, 8, 15,16,17,18,19,20,21,22] were included in our studies (Fig. 1).The main characterizes of included studies were summarized in Table 1. In terms of quality, among four RCT studies, One study have low risk of bias, two studies showed unclear risk of bias and two studies showed high risk of bias. The remaining 6 non-RCTs all scored highly (with five stars or more) by NOS (Table S1 and S2).
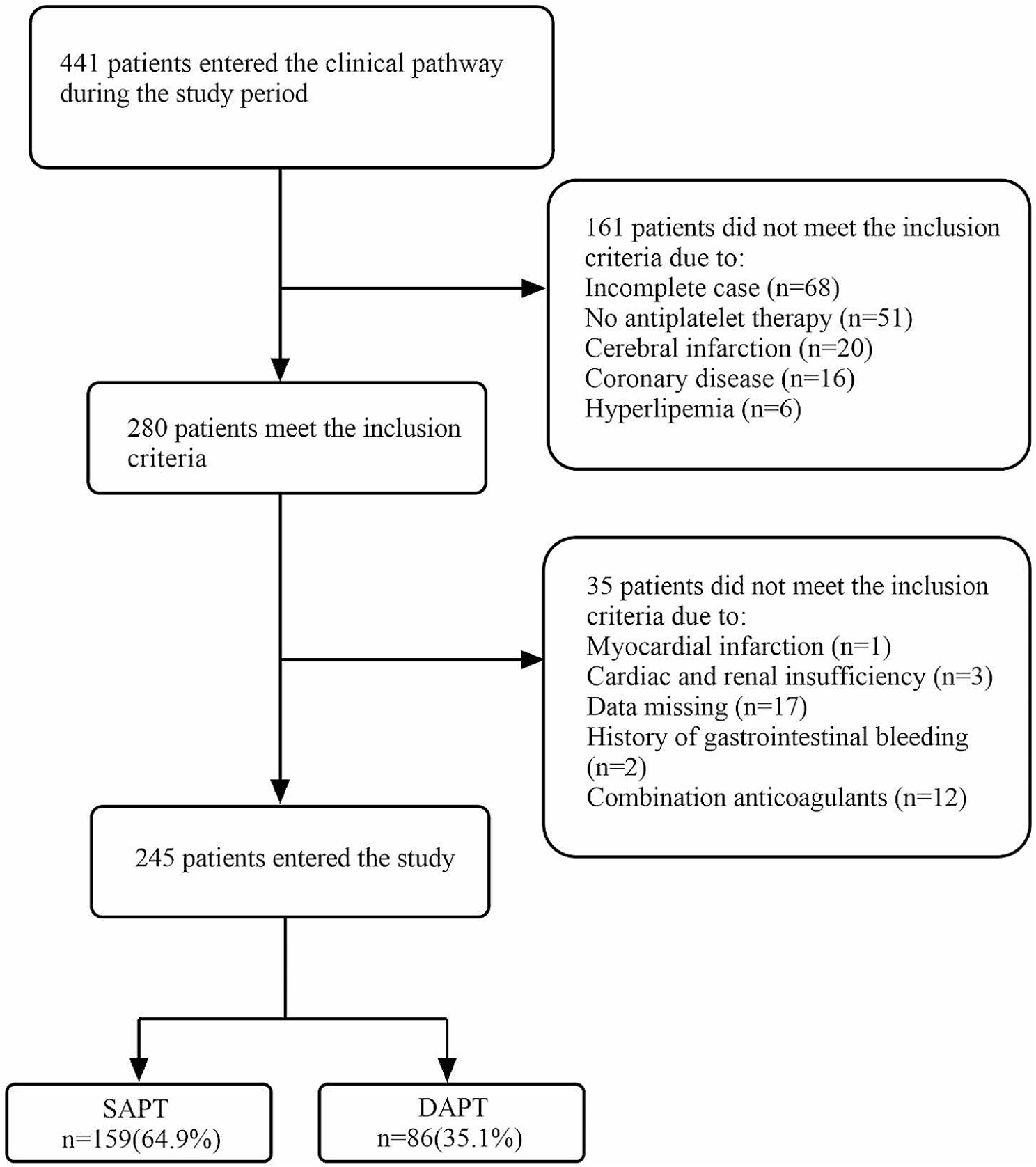
Fig. 1Flow diagram of studies selection procedure
Table 1 Main characteristics of all studies included in the meta-analysisABP reduced the pneumothorax rate when compared with control groups.
All included 10 studies including 3874 patients (1904 cases and 1970 controls) evaluated the relationship between ABP and pneumothorax rate. The pooled analysis suggested that ABP was significantly associated with lower pneumothorax rate when compared with control (incidence: 20.0% vs. 27.9%, OR = 0.57, 95% CI = 0.48–0.66, P < 0.001) (Fig. 2; Table 2).
Fig. 2Forest plot of the association between ABP use and pneumothorax rate after CT-PTLB
Table 2 Main meta-analysis results of ABP procedure in patients receiving CT-PTLBAs patients with emphysema were more easily to develop pneumothorax after CT-PTLB, we collected datasets to evaluate whether ABP could also reduce pneumothorax incidence in patients with emphysema. Finally, four studies evaluated the role of ABP in patients with and without emphysema. The pooled analysis suggested that although the incidence of pneumothorax in patients with emphysema was higher than in those without emphysema, the use of ABP could reduce pneumothorax incidence in not only patients without emphysema (incidence: 20.1% vs. 31.2%, OR = 0.51, 95% CI = 0.33–0.79, P = 0.002) (Fig. 3B) but also in patients with emphysema (incidence: 30.0% vs. 49.8%, OR = 0.37, 95% CI = 0.19–0.72, P = 0.004) (Fig. 3A).
Fig. 3Forest plot of the association between ABP use and pneumothorax rate in patients with emphysema (A) and without emphysema (B) after CT-PTLB
Subgroup analysis according to study type was done. We found the pooled result of both 4 RCTs and the remaining 6 retrospective studies showed the use of ABP could significantly reduce the incidence of pneumothorax (for RCTs, incidence: 23.2% vs. 34.2%, OR = 0.58, 95% CI = 0.35–0.95, P = 0.005; for retrospective studies, incidence: 19.4% vs. 26.8%, OR = 0.56, 95% CI = 0.47–0.67, P < 0.001)(Table 2).
ABP technique applied in our study could be classified as clotted and non-clotted blood. The studies applied clotted blood were all RCTs and the remaining studies applied non-clotted blood were all retrospective studies, as a consequence, the result was the same as in the subgroup analysis according to study type, both clotted and non-clotted blood technique could reduce the incidence of pneumothorax after CT-PTLB (Table 2).
ABP reduced the chest drain insertion rate when compared with control groups.
Nine studies with 3006 patients (1485 cases and 1521 controls) evaluate the relationship between ABP and the chest tube insertion rate. The patients with ABP was associated with lower chest tube insertion rate when compared with control groups (4.0% vs. 8.0%, OR = 0.47, 95% CI = 0.34–0.65, P < 0.001) (Fig. 4). Subgroup analysis by study type (RCTs and retrospective studies) and type of ABP technique (clotted and non-clotted blood patch) all found significantly reduced chest tube insertion rate in ABP group when compared with control group (Table 2).
Fig. 4Forest plot of the association between ABP use and chest tube insertion rate after CT-PTLB.
HeterogeneityNo large heterogeneity (I2 ≥ 65%) was detected in the all analysis. In pneumothorax rate analysis, we found moderate heterogeneity in the subgroup analysis according to emphysema status (I2 for absent = 28%, I2 for present = 47%), research type (I2 for RCT = 37%) and type of ABP (I2 for clotted = 37%). In chest drain insertion rate analysis, studies with RCT and clotted ABP showed moderate heterogeneity (I2 = 43).As a result, random effect model (DerSimonian and Laird) analysis was applied. Except this, no significant heterogeneity was detected in other comparisons and the fixed-effect model (the Mantel Haenszel method) was used.
Sensitivity analysis.
In the sensitivity analysis, the influence of each study on the pooled OR on pneumothorax rate and chest tube insertion rate was examined by repeating the meta-analysis while omitting each study one at a time. The analysis results suggested that no individual study significantly affected the pooled OR, suggesting our result was robust and reliable (Fig. 5A and B).
Fig. 5Sensitivity analyses omitting one study each time on the influence of ABP use and pneumothorax rate (A) and chest tube insertion rate (B) after CT-PTLB
Fig. 6The funnel plot of the meta-analysis of the impact of ABP on pneumothorax (A) and chest tube insertion rate (B) in patients after CT-PTLB.
Publication biasNo significant bias was indicated by the Begg’s and Egger’s test (pneumothorax rate: PBegg = 0.47, PEgger = 0.32; chest tube insertion rate: PBegg = 0.39, PEgger = 0.18).
留言 (0)