
記住我





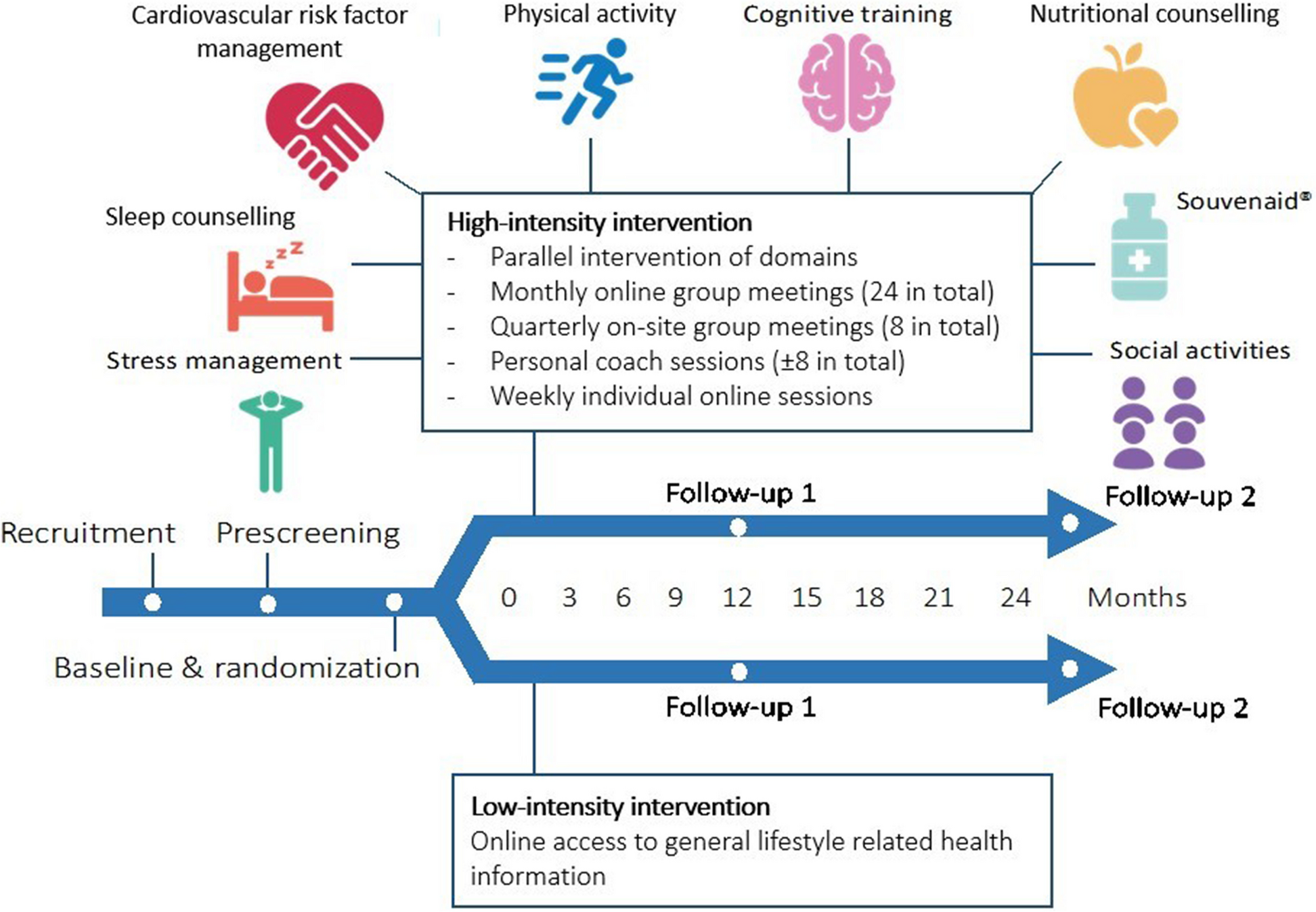
FINGER-NL is a multi-center, randomized, controlled, multidomain lifestyle intervention trial among 1,210 older adults at risk for cognitive decline, with a duration of 24 months. Block-randomization stratified by study site (block sizes of preferably 20–24 participants) was used to centrally allocate eligible participants in a 1:1 ratio to a personalized multidomain lifestyle intervention (HI-group) versus online access to general lifestyle-related health information (LI-group). The multidomain intervention comprises a combination of 7 lifestyle components (physical activity, cognitive training, cardiovascular risk factor management, nutritional counseling, sleep counseling, stress management, social activities) and a nutritional product (Souvenaid, 125 mL). The study is conducted in five study centers across The Netherlands (Amsterdam, Groningen, Maastricht, Nijmegen, Wageningen). Outcome measurements are conducted at baseline, 12 months (Follow-up 1) and 24 months (Follow-up 2) after randomization. A flow-chart of the study design is shown in Fig. 1. FINGER-NL is part of the ‘Maintaining Optimal Cognitive Function In Ageing’ (MOCIA) research program (https://mocia.nl/scientific/).
Fig. 1
Summary of the FINGER-NL study design
Recruitment of participantsParticipant recruitment took place via the online recruitment platform Dutch Brain Research Registry (https://hersenonderzoek.nl/) which supports recruitment and pre-screening of research volunteers for neuroscience studies through a fully online registry [22]. In parallel, study sites used their own local participant pools and deployed initiatives for additional recruitment.
Inclusion criteriaInclusion criteria were (1) age 60–79 years at pre-screening; (2) adequate fluency in Dutch to understand the informed consent and complete study questionnaires; (3) informed consent to all study procedures; (4) Internet access at home; (5) presence of ≥ 3 self-reported risk factors for cognitive decline (including at least 2 modifiable risk factors and 1 non-modifiable risk factor). Modifiable risk factors include self-reported presence (based on a single question) of risk factors [23, 24].
Modifiable risk factors:
- Physical activity
- Unhealthy diet
- Low mental/cognitive activity
- High blood pressure
- High cholesterol
- High body mass index (defined as ≥ 25 kg/m2 for 60–69 years old, and ≥ 28 kg/m2 for ≥ 70 years old, based on self-reported height and weight)
Non-modifiable risk factors:
- First-degree family history of dementia
- Subjective cognitive decline/memory complaints
Exclusion criteriaExclusion criteria were: (1) self-reported diagnosis of dementia or mild cognitive impairment; (2) cognitive impairment assessed by the Modified Telephone Interview for Cognitive Status battery (TICSm score < 23) [25]; (3) conditions affecting safe and continuous engagement in the intervention (e.g. under treatment for current malignant diseases), major psychiatric disorders (e.g. major depression, psychosis, bipolar disorder), neurological disorders thought to interfere with cognitive function (e.g. Parkinson’s disease, multiple sclerosis), symptomatic cardiovascular disease (e.g. stroke, angina pectoris, heart failure, myocardial infarction), re-vascularization within the last three months, severe loss of vision, impaired hearing or communicative ability, severe mobility impairment, other conditions preventing co-operation as judged by the local study nurse or consulted physician at the local study site; (4) simultaneous participation in any other intervention trial at time of pre-screening; (5) participation in FINGER-NL of another household member to prevent contamination.
Online (automatic) prescreening and telephone prescreeningOnline (automatic) prescreening was performed in potentially eligible participants recruited through the Dutch Brain Research Registry according to inclusion and exclusion criteria (except for TICSm score) to reduce screen failures. For individuals recruited through local cohorts, manual prescreening was performed based on available information on inclusion and exclusion criteria. On first contact, participants received the screening information letter, study information letter and informed consent form. In a second step, interested participants underwent an eligibility-check and a brief cognitive assessment (TICSm) via telephone screening performed by the five FINGER-NL study sites [25]. If participants fulfilled all study criteria, they were invited for an on-site baseline visit.
Randomization and blindingParticipants were randomized after providing written informed consent and after completing the baseline visit. Participants were allocated randomly into either the HI-group or the LI-group using a computer random number generator with randomly varied permuted blocks of 4 to 6 and an equal 1:1 allocation ratio, stratified by study site. Randomization took preferably place per 24 participants per site simultaneously, resulting in balanced HI-groups and LI-groups of 12 participants each and equal starting point of the intervention. To promote blinding and adherence, and inspired by U.S. POINTER [26], we deliberately avoid the label ‘control group’, but rather designate both groups as receiving some form of lifestyle intervention, differing however in structure and intensity. Personnel collecting the primary outcome measures (cognition) and researchers conducting the statistical analyses are blinded to group allocation.
Intervention programHigh-intensity interventionThe HI-group follows a personalized, supervised and hybrid intervention, addressing a combination of 7 lifestyle components and 1 nutritional product. The 2-year intervention consist of 24 monthly online group meetings (duration: 90-min; 2–4 lifestyle domains addressed each meeting) and 8 three-monthly group meetings at the study site (duration: 120 min; 4–5 lifestyle domains addressed each meeting), all guided by a lifestyle coach, resulting in a total of 32 group meetings. The group meetings are supplemented with 6 individual sessions with a lifestyle coach to personalize the intervention (phone/video consultations; duration: 10–60 min; one or more specific lifestyle domains addressed each meeting depending on the needs and goals of the participant following the principles of motivational interviewing). Finally, participants have access to a digital intervention platform to engage in individual online sessions (duration: 5 min up to four hours per week) and access to additional, carefully selected or custom-made training material (e.g. videos, apps) throughout the intervention period. To avoid overload and foster adherence, lifestyle components are initiated in a stepwise manner and the burden of the intervention is deliberately distributed over 24 months. See Table 1 and Additional file 1 for an overview of all intervention domains and activities. Each group is guided through the intervention by a local intervention team, consisting of an experienced lifestyle coach and a study navigator. The (certified) lifestyle coach is responsible for the actual execution of all intervention modules and activities as well as personalizing the intervention. Professional profiles differed, but the majority of lifestyle coaches was physiotherapist or dietitian. The study navigator (no specific background; e.g., study nurse or junior researcher) is the site-specific primary contact point for participants and provides (ad-hoc) individual support and ongoing encouragement to achieve maximum adherence and reduce dropouts.
Table 1 Overview of lifestyle domains in the FINGER-NL high-intensity and the low-intensity groupLow-intensity interventionThe LI-group receives general lifestyle-related health information covering all domains of the high-intensity intervention except the nutritional product. In the course of the study duration, 14 information leaflets are shared with participants, i.e., one in each intervention year for each of the seven lifestyle intervention domains (see Table 1). The information leaflets are provided via the digital intervention platform.
Digital intervention platformTo improve trial efficiency (and in anticipation of possible (future) COVID-19 restrictions which were still highly probable at the time of study start), participants have access to a personal intervention environment via a digital platform (Ivido). This digital platform is used to facilitate the trial workflow and execution of the intervention. Participants in the HI-group have access to: (1) a personal landing page/dashboard including a general overview of participants’ personal health profile); (2) online aspects of the intervention (e.g. video instructions for home exercise, training material, videos, weekly information or motivational snippets to boost adherence) and receive personalized information and easy access to integrated applications which support the intervention; (3) chat function to communicate with the research team; (4) insight into intermediate outcomes (e.g. blood pressure, body mass index (BMI)). Furthermore, the platform is used for data-collection such as the administration of questionnaires/measurements and to measure adherence to the several intervention domains (e.g. number of tasks completed). For participants in the LI-group access to the online dashboard is limited to general lifestyle-related health information and administration of questionnaires/measurements.
To foster adherence, both groups receive regular newsletters via e-mail. At the two follow-up outcome measurements, participants receive small gift vouchers (€10-€20).
Baseline and outcome measurementsAll study participants undergo a baseline measurement and two follow-up outcome measurements at 12 months (follow-up 1) and 24 months (follow-up 2) after randomization at the research site. The baseline and follow-up outcome measurements include an assessment of demographics (e.g., age, gender, level of education, socioeconomic status; baseline only), medical history and medication (including items on smoking and alcohol consumption), cognitive testing, clinical measures, blood sampling (e.g., APOE e4 carriership) and questionnaires (See Table 2). At baseline only, we used the Montreal Cognitive Assessment (MOCA) to assess global cognitive performance [27]. All measurements/tests were administered by trained personnel. For personnel collecting the primary outcome measures (cognition) regular intervision meetings were set up.
Table 2 FINGER-NL data-collectionPrimary outcomeThe primary outcome is the 2-year change from baseline in a global cognitive composite score derived from subtest scores from the neuropsychological test battery (NTB). The NTB includes (i) 15-Word Verbal Learning Test delayed recall (episodic memory) [28], (ii) Digit Symbol Substitution Test 90 seconds (processing speed) [29], (iii) Wechsler Adult Intelligence Scale digit span backwards [30], and (iv) semantic fluency (animals; both attention and executive functions) [31, 32]. The choice for this subset was based on consultations with neuropsychologists to cover the cognitive domains attention and executive functioning, processing speed and memory, their sensitivity to early cognitive changes in older individuals, administration time, and suitability for harmonization with other large multidomain intervention studies. The raw scores of individual tests will be transformed into standardized z-scores using the cohort-wide means and standard deviations (SD) at baseline (with higher scores suggesting better performance). The NTB total score is obtained by averaging the z-scores of the four individual tests and re-standardization. The minimum number of necessary individual tests was set to 3 out of 4 for calculating the NTB total score.
Secondary outcomesSecondary outcome measurements include 2-year change on the individual cognitive test performances (see above), instrumental activities of daily living (Amsterdam Instrumental Activity of Daily Living Questionnaire (A-IADL-Q) [33]), quality of life (5-level EuroQol-5D (EQ-5D-5L) [34]), modifiable dementia risk (‘LIfestyle for BRAin health’ (LIBRA) score [23, 24]), and several intervention-specific outcomes (physical activity (maximum grip strength, physical activity (SQUASH questionnaire [35]), sedentary behavior (LASA Sedentary Behavior Questionnaire [36]) and sarcopenia (SARC-F Sarcopenia Questionnaire [37])), fatigability (Pittsburgh Fatigability Scale [38]), 7 days Accelerometry (ActiGraph GT9X) combined with 7 days Physical Activity Record (Groningen study site only), cognitive training (cognitive function, meta-memory (Meta-memory in Adulthood Questionnaire [39])), cardiovascular risk factor management (blood pressure, cholesterol (total, HDL, LDL + triglycerides), blood glucose (HbA1c), waist circumference, BMI, medication adherence (Hill-Bone Medication Adherence Scale [40])), nutritional counselling (nutritional intake (Traqq app [41]), adherence to MIND-NL-Eetscore Food Frequency Questionnaire [42]), sleep counselling (sleep behavior (7-day sleep diary), insomnia (Insomnia Severity Index [43])), stress management (mindfulness (Five Facet Mindfulness Questionnaire [44]), perception of stress (Perceived Stress Scale [45])), and social activities (perceived social support (Lubben Social Network Scale [46]), emotional and social loneliness (De Jong Gierveld Loneliness Scale [47])). In addition, we will analyze blood-based biomarkers for Alzheimer’s disease (Aβ42/40, p-tau), axonal damage (NfL), astrocytes activity/injury or stress (GFAP) and brain plasticity (BDNF).
Exploratory outcomes (heterogeneity of treatment effects)As an exploratory analysis, we investigate whether the effectiveness of the intervention with respect to the primary and secondary cognitive outcomes is modified by demographics (age, gender, years of education, socioeconomic status), baseline LIBRA score, baseline cognitive performance (MOCA), baseline scores of the Motivation to Change Lifestyle and health Behaviours for Dementia Risk Reduction scale, APOE e4 carriership, presence of a first-degree relative with dementia, presence of subjective cognitive decline/memory complaints and blood-based biomarkers for Alzheimer’s disease.
Sample sizeSample size calculation was based on the primary outcome (NTB total score). In the original FINGER trial [8], an effect size of 0.127 (Cohen’s d) was reported for the 2-year change from baseline on the NTB total score following a multidomain lifestyle intervention. In the LipiDiDiet trial [13], an effect size of 0.17 (Cohen’s d) was reported for the 2-year change from baseline on the NTB total score following an intervention with Souvenaid. As FINGER-NL combines a multidomain lifestyle intervention with Souvenaid, an effect size (Cohen’s d) of 0.20 (SD = 1) for NTB total score was anticipated for the 2-year change from baseline on the NTB total score in the HI-group compared to the LI-group. With a power of 90%, 2-sided significance level of α = 0.05 and an anticipated drop-out rate of 12.5%, a total of 1,206 subjects (603 per group after randomization) was considered adequate to detect the desired effect size.
Statistical analysesIn alignment with other WW-FINGERS studies, we will test for change in the primary and secondary outcome variables, both within-group and between-group using linear mixed models with random effects for intercept (individuals) and slope (time). Time and randomization group will be entered as fixed effects, study site will be included as fixed covariate. Change in the outcome variables will be modelled by including the interaction term between randomization group and time as fixed effect. The intention-to-treat principle will be used. Missing primary and secondary outcome data will be handled through restricted maximum likelihood (REML) estimation of expected scores in the mixed models. Given the size of FINGER-NL, no additional covariates will be included in the primary model, and differences between individuals will be treated as random nuisance parameters in the REML model [48]. For the primary outcome, the level of significance will be set at 0.05 (two-sided). The Benjamini–Hochberg correction will be used to account for multiple comparisons of correlated secondary and exploratory outcomes.
留言 (0)