
記住我
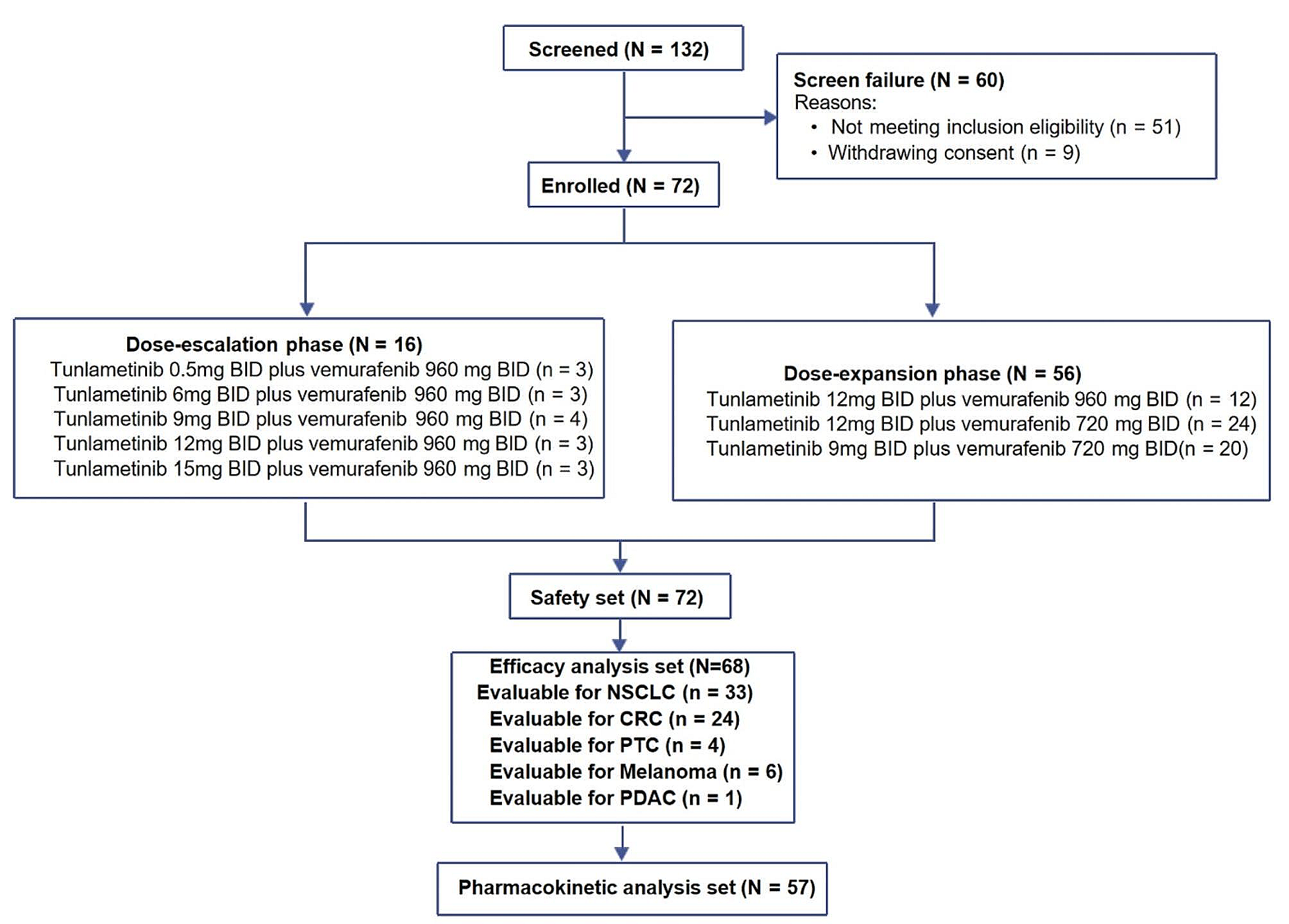


From August 17, 2018 to April 19, 2022, a total of 72 patients with BRAF V600-mutant solid tumors were enrolled; the data cut-off date of this study was December 15, 2023. Patient disposition is presented in Fig. 1, and the demographic and baseline characteristics are presented in Table 1. All patients have completed the 12 weeks of treatment or discontinued treatment caused by disease progression, unacceptable toxicity, withdrawal of consent, or death. The median duration of treatment was 5.3 months (Q1-Q3: 2.7–8.6). Among all patients enrolled, the tumor types included NSCLC (n = 36, 50.0%), CRC (n = 25, 34.7%), melanoma (n = 6, 8.3%), PTC (n = 4, 5.6%), and pancreatic cancer (n = 1, 1.4%). The median duration of treatment was 4.4 months (Q1-Q3: 2.5–8.2) for tunlametinib and 4.3 months (Q1-Q3: 2.5–7.2) for vemurafenib. Demographic and baseline characteristics by dose group are listed in Supplementary Table S1 (online only).
Fig. 1
Study design and patient disposition. All dose groups were given study drug treatment twice daily (BID). BID, Bis In Die; CRC, colorectal cancer; NSCLC, non-small cell lung cancer; PTC, papillary thyroid carcinoma; PDAC, pancreatic ductal adenocarcinoma
Table 1 Demographic and baseline characteristicsIn 36 patients with NSCLC enrolled across the dose-escalation and the dose-expansion phases, the median duration of treatment was 5.7 months (Q1-Q3: 3.7–11.8) for tunlametinib and 5.7 months (Q1-Q3: 3.7–11.0) for vemurafenib. In the FAS of 33 patients with evaluable disease, 45.5% (15/33) patients had received prior systemic antitumor therapy, and 54.5%(18/33) patients were treatment naïve. Demographic and baseline characteristics for the NSCLC cohort by dose group are listed in Supplementary Table S2 (online only).
In 25 patients with CRC, the median duration of treatment was 5.6 months (Q1-Q3: 2.7–7.6) for tunlametinib and 5.6 months (Q1-Q3: 2.7–7.6) for vemurafenib. Twenty-four (96.0%) patients with CRC had received prior antitumor therapy.
Of the 4 patients with PTC, all were radioactive iodine-refractory differentiated thyroid cancer (RAIR-DTC), the median duration of treatment was 4.7 months (Q1-Q3: 1.7–10.3) for tunlametinib and 3.5 months (Q1-Q3: 1.7–6.3) for vemurafenib.
6 patients of Melanoma had all previously treated with systemic therapy (interferon, or dacarbazine plus cisplatin etc.). The median duration of treatment was 2.9 months (Q1-Q3: 0.8-5.0) for tunlametinib and 2.9 months (Q1-Q3: 0.8–7.7) for vemurafenib.
1 patient with pancreatic cancer, whose pathology type was pancreatic ductal adenocarcinoma (PDAC), this patient was previously heavily treated. The median duration of treatment was 3.5 months for both tunlametinib and vemurafenib.
SafetyNo DLTs occurred across all dose groups in the dose-escalation phase, and the MTD was not reached. All 72 patients in the dose-escalation and dose-expansion phases were included in the SS. The most common TRAEs were anemia (61.1%, 44/72), blood creatine phosphokinase increased (56.9%, 41/72), and rash (54.2%, 39/72). The incidence of ≥ grade 3 TRAEs was 59.7% (43/72) and serious TRAEs was 31.9% (23/72; Supplementary Table S3, online only) across all doses. A summary of TRAEs ≥ 15% is listed in Table 2. The most frequent ≥ grade 3 TRAEs were anemia (18.1%, 13/72) and blood creatine phosphokinase increased (13.9%, 10/72). Among all TRAEs, 16.7% (12/72) were reported with ejection fraction decreased, 15.3% (11/72) patients with blurred vision, and 12.5% (9/72) with QT interval prolongation.
Table 2 Incidence of TRAEs ≥ 15% (by preferred term)11.1% (8/72) patients experienced TRAEs leading to study drug discontinuation, most occurred in the tunlametinib 12 mg BID plus vemurafenib 960 mg BID and tunlametinib 15 mg BID plus vemurafenib 960 mg BID dose groups (Supplementary Table S3, online only). The most common TRAE leading to study drug discontinuation was ejection fraction decreased (2.8%, 2/72). 6.9% (5/72) patients experienced TEAEs leading to death, including 2 deaths due to poor basic cardiopulmonary function, 2 due to disease progression and 1 due to sudden death. One report of sudden cardiac death was considered related to the study drug treatment of tunlametinib 12 mg BID plus vemurafenib 720 mg BID, as assessed by the investigator. Other deaths were considered not related to the study drug treatment, as assessed by the investigators.
During cycle 2–4, TRAEs leading to study drug discontinuation were reported in 26.7% (4/15) of patients in the tunlametinib 12 mg BID plus vemurafenib 960 mg BID dose group and over 50% of patients experienced a TRAE leading to dose adjustment in the tunlametinib 12 mg BID plus vemurafenib 720 mg BID dose group.
In the tunlametinib 9 mg BID plus vemurafenib 720 mg BID dose group of NSCLC patients, the incidence of ≥ grade 3 TRAEs were 35.3% (6/17) and serious TRAEs were 29.4% (5/17); the ORR, median DoR, and median PFS were 60.0% (95% CI, 32.3–83.7), 11.3 months (95% CI, 3.9-NE), and 10.4 months (95% CI, 5.6-NE), respectively. Therefore, the tunlametinib 9 mg BID plus vemurafenib 720 mg BID group was determined as the RP2D for patients with BRAF V600-mutant NSCLC according to the better tolerability and consistent efficacy compared with the other study drug dose groups.
Efficacy.
The efficacy outcomes of NSCLC patients are shown in Table 3; Fig. 2, and Fig. 3; efficacy outcomes of CRC, PTC, melanoma and PDAC patients are presented in Supplementary Table S4 and Supplementary Fig S1 and Fig S2 (online only). The swimmer and waterfall plots of all patients are presented in Supplementary Fig S3 (online only).
Table 3 Efficacy of tunlametinib plus vemurafenib in NSCLC patients with evaluable diseaseFig. 2
Tumor responses in NSCLC patients with evaluable disease. (A) Waterfall plot of best percentage change from baseline in total sum of target lesion diameters. (B) Swimmer plot of best percentage change from baseline in total sum of target lesion diameters. (C) Spider plot of percentage change from baseline in total sum of target lesion diameters. All dose groups were given study drug treatment twice daily(BID). BID, Bis In Die; CR, complete response; NE, not evaluable; NSCLC, non-small cell lung cancer; PD, progressive disease; PR, partial response; SD, stable disease
Fig. 3
Kaplan–Meier curve for NSCLC patients. (A) progression-free survival in NSCLC patients; (B) duration of response in NSCLC patients. All dose groups were given study drug treatment twice daily (BID). BID, Bis In Die; CI, confidence interval; DoR, duration of response; NE, not evaluable; NSCLC, non-small cell lung cancer; PFS, progression-free survival
NSCLC patientsAmong 36 NSCLC patients, three patients were excluded from the FAS due to lack of baseline target lesions. Of 33 patients with baseline target lesions included in the FAS, 6.1% (2/33) achieved complete response (CR), 54.5% (18/33) achieved partial response (PR), and 27.3% (9/33) experienced stable disease (SD). Patients with CR and PR contributed to an ORR of 60.6% (20/33; 95% CI, 42.1–77.1) and those with CR, PR, and SD contributed to a DCR of 87.9% (29/33; 95% CI, 71.8–96.6) (Table 3). The median DoR was 11.3 months (95% CI, 6.8-not evaluable [NE]); the median PFS was 10.5 months (95% CI, 5.6–14.5) for all NSCLC patients (Fig. 3). For the RP2D of tunlametinib 9 mg BID plus vemurafenib 720 mg BID dose group, the ORR, median DoR, and median PFS were 60.0%, 11.3 months (95% CI, 3.9-NE), and 10.5 months (95% CI, 5.6-NE) respectively (Table 3 and Supplementary Fig S1, online only).
Among 15 patients who had received prior systemic antitumor therapy, 8 achieved PR, the ORR was 53.3% (8/15; 95% CI, 26.6–78.7); in 18 patients who were treatment naïve, 12 achieved PR, the ORR was 66.7% (12/18; 95% CI, 41.0-86.7).
CRC patientsOf 24 CRC patients with evaluable disease, six achieved PR and 15 experienced SD. The ORR was 25.0% (6/24; 95% CI, 9.8–46.7) and the DCR was 87.5% (21/24; 95% CI, 67.6–97.3, Supplementary Table S4, online only). The median DoR was 5.5 months (95% CI, 2.9-NE) and the median PFS was 6.2 months (95% CI, 4.8–7.6) (Supplementary Fig S2, online only).
PTC patientsOf four patients with PTC, 50.0% (2/4) achieved PR and 50.0% (2/4) experienced SD (Supplementary Table S4 and Fig S1, online only).
In addition, 6 patients with melanoma exhibited varying degrees of tumor shrinkage. And one patient with PDAC achieved PR.
PKA total of 57 patients were included in the PK analysis set. After single-dose administration, tunlametinib plasma concentration increased rapidly and declined slowly. The maximum concentration (Cmax) and area under the concentration–time curve (AUC) increased generally in a dose-dependent manner. After multiple administrations, the average accumulation ratio ranged from 0.7 to 3.0 based on Cmax, 1.6 to 4.3 based on AUCtau, and 1.6 to 3.5 based on AUClast across doses (Supplementary Table S5, online only).
After single-dose of vemurafenib, vemurafenib was absorbed slowly with median time to maximum plasma concentration (Tmax) of approximately 4 h and then declined slowly. After multiple administrations of vemurafenib, the average accumulation ratio ranged from 8.2 to 16.0 based on Cmax, 13.3 to 14.1 based on AUCtau, and 10.6 to 36.3 based on AUClast across doses (Supplementary Table S6, online only).
No drug–drug interaction was identified between tunlametinib and vemurafenib.
留言 (0)