
記住我





Acute myocardial infarction (AMI) represents a consequence of ischemic heart diseases (IHD), mainly caused by the partial or the complete blockage of the epicardial coronary arteries leading to the death of myocardial cells. These cells are replaced by fibrotic tissue, resulting in a loss of cardiac contractility. AMI accounts for over 33% of mortality associated with IHD [1]. It can be classified into two types: ST-segment elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI), based on the electrocardiographic presentation during diagnosis. The severity of ST-segment changes is influenced by the location of the myocardial region affected by acute ischemia [2, 3]. Patients with STEMI are at higher risk of mortality due to complete thrombotic occlusion of the vessel, transmural infarction, and the absence of collateral circulation [4]. On the other hand, patients with non-STEMI experience reduced blood flow in the affected coronary artery without complete occlusion, but they face higher long-term mortality risk due to the potential occurrence of multivessel coronary artery disease [5]. Throughout this review, we will focus mainly on STEMI cases because the total occlusion of the vessel greatly impacts on the biochemical pathways of interest, highlighting them. The ischemic episode is primarily caused by plaque rupture, leading to the formation of blood clots that reduce microcirculatory perfusion and limit blood flow to the heart. This imbalance between oxygen supply and demand accounts for about 70% of fatal events [6]. Then, reperfusion strategies, such as pharmacological approaches or percutaneous coronary intervention (PCI) and coronary artery bypass, have become the gold standard for treating AMI [6].
Early reperfusion has been demonstrated to limit ischemic cell death, but it can also result in cellular alterations and further tissue damage. The resulting damage can be categorized as reversible or irreversible. Reversible damage allows cardiac myocytes in the affected area to survive ischemia, and early reperfusion facilitates the recovery of cellular function. However, irreversible damage causes complete loss of resilience in myocytes, leading to cardiac tissue death. Irreversible damage is characterized by various changes in cardiomyocyte structure, including cell swelling, denaturation of intracellular proteins, and cell calcification [7]. During hypoxia, cardiomyocytes undergo anaerobic metabolism, leading to ATP production deficiencies, ion imbalances, and intracellular acidosis. Upon blood flow restoration, rapid reoxygenation of cardiac tissue restores ATP production and pH levels but also leads to the hyperproduction of reactive oxygen species (ROS) and intracellular calcium (Ca2+) overload, ultimately causing cardiomyocyte death and systolic dysfunction [8]. Arrhythmogenesis, whose onset is very common after ischemia and at reperfusion time, represents one of these dysfunctions. Here, mitochondria might have a central role through the control of the metabolism-excitation route, despite it is not yet fully clarified. Indeed, some mitochondrial-localized channels (i.e., inner membrane anion channel) when inhibited help in maintaining the mitochondrial membrane potential (ΨM) and action potentials during stress. Moreover, also Ca2+ and (mitochondrial ROS) appear to be determinant, by promoting mitochondrial dysfunctions dependent from a vicious cycle of Ca2+ overload and mitoROS production, consequent Ryanodine receptor 2 (RyR2) oxidation and Ca2+ leak from the sarcoplasmic reticulum (SR) [9].
As a messenger of cell death, but also stimulator of ATP synthesis and cardiac contraction [10], Ca2+ is sensed and captured by mitochondria from different intracellular stores (i.e., SR) and the extracellular milieu (Fig. 1). The events associated with ischemia reperfusion (I/R) have a strong impact on Ca2+ homeostasis, causing a variation in the expression and functionality of the proteins that bind and transport Ca2+; therefore, these changes in the intracellular Ca2+ fluxes can influence cell fate.
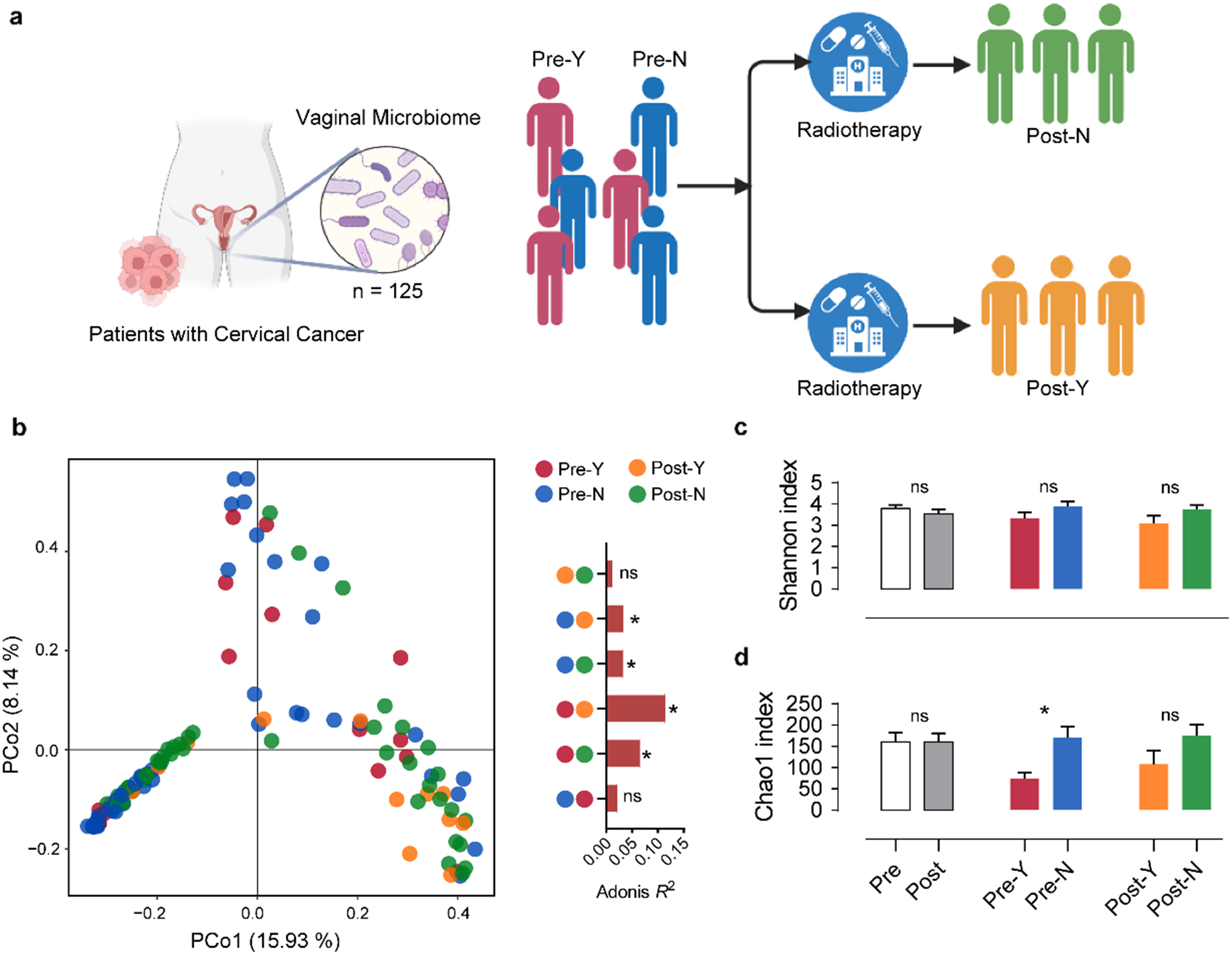
Fig. 1
Representation of the Ca2+ signaling between mitochondria and sarcoplasmic reticulum in healthy condition and after IRI
This figure illustrates the dynamics of calcium (Ca2+) signaling between the sarcoplasmic reticulum (SR) and mitochondria associated membranes (MAMs) under normal physiological conditions and following ischemia-reperfusion injury (IRI). In healthy conditions, Ca2+ ions are released from the SR via channels such as the inositol 1,4,5-triphosphate receptor type 3 (IP3R3), inositol 1,4,5-triphosphate receptor type 1 (IP3R1), and ryanodine receptors (RyR2). These Ca2+ ions can then enter the mitochondria through the voltage-dependent anion-selective channel (VDAC) and the mitochondrial calcium uniporter (MCU). Following IRI, alterations in Ca2+ handling occur, affecting the balance between the SR and mitochondria. This dysregulation may involve changes in the activity of the Na+/ Ca2+ exchanger (NCX), plasma membrane Ca2+ ATPase, and sarcoplasmic reticulum Ca2+ ATPases (SERCA), as well as modulation of the phosphorylation status of phospholamban (PLB). Disruption of Ca2+ homeostasis during IRI can lead to mitochondrial dysfunction such as excessive reactive oxygen species (ROS) production, mPTP opening, impairment of ATP production and cell death
In this review, we will summarize the impairments in charge of mitochondria, SR and their contact sites named as mitochondria associated membranes (MAMs), that could be clinically relevant in cardiac I/R. We will highlight biochemical events regarding Ca2+ signaling dysregulation as contributor of cardiac damage, and whether they can be successfully targeted to reduce reperfusion injury. Despite advancements, patients with AMI continue to face substantial risks of mortality and morbidity. Novel treatments are imperative to shield the myocardium from the adverse impacts of AMI and reperfusion injury, aiming to minimize infarct size (IS), to sustain cardiac function, and to forestall heart failure onset [11, 12].
The importance of sarcoplasmic reticulum and mitochondria for Ca2+ homeostasis in acute myocardial infarctionThe balance of intracellular Ca2+ at any level is crucial for normal cardiomyocyte function, from embryos to adulthood [13]. One of the main functions of the sarcoplasmic reticulum (SR) is to finely regulate the accumulation and the release of this ion close to the subsarcolemmal space, playing a key role in excitation-contraction coupling (ECC) in the heart. The importance of Ca2+ handling at SR and T tubules (TT) interface in ECC is widely reviewed elsewhere and it is already a reliable molecular target for cardioprotective drugs. What is almost unknown to date is the contribution of the dysregulation of Ca2+ signaling at the SR-mitochondria interface in ECC. Indeed, whether this pattern is essential for cardiac excitation-metabolism coupling, still few evidence connects mitochondria Ca2+ buffering to heart contraction. A seminal paper by Rizzuto’s group, in 2012 provided the first pioneer proof that mitochondria are able to taken up a significant fraction of Ca2+ released during systole and then released back into the cytosol during diastole [14]; this happens through the mitochondrial calcium uniporter (MCU) complex, a channel of the inner mitochondrial membrane (IMM). Moreover, the MCU-mediated Ca2+ uptake into mitochondria is of crucial importance for the direct ATP synthesis [15] and for the activation of dehydrogenases that feed electrons into the respiratory chain. Of note, MCU is essential for the control of “fight or flight” mechanisms, by regulating the Ca2+-mediated heart rate increase in cardiac pacemaker cells during stress [16]. Further investigations encompassing these noteworthy findings have been poor in the pathological field perhaps leaving the real role of the mitochondrion in ECC unknown. As mitochondria receive Ca2+ from SR, cytosol and from microdomains that are formed at MAMs, essential is the evaluation of what changes in correspondence of this route during AMI.
The proximity between mitochondria and SR facilitates reciprocal exchange between organelles, enabling tight integration between ATP generation by mitochondria and Ca2+ release mediated by Ca2+ channels in SR membrane, meeting the energy demands of the myocyte [17]. The activity of various mitochondrial enzymes in oxidation is influenced by the concentration of Ca2+, suggesting that an increase in Ca2+ influx into mitochondria promotes electron transport and ATP production. Indeed, it is reported that tricarboxylic acid (TCA) cycle is modulated by Ca2+ levels, in particular, the activation of ketoglutarate dehydrogenase (KGDH), isocitrate dehydrogenase (IDH) and pyruvate dehydrogenase (PDH) are directly dependent from matrix Ca2+ concentration [18, 19]. This leads to an increase in NADH, higher activity of the ETC and a positive loop for what concern mitochondrial metabolism. An additional dehydrogenase, named as FAD-glycerol phosphate dehydrogenase (GPDH) and localized in the IMM, mediates the transfer of reducing equivalents from NADH to the ETC by increasing ATP production [20, 21].
Overall, evidence of the Ca2+-dependent modulation of the oxidative phosphorylation derived by studies on skeletal muscle, which described an augmentation of conductance of the complexes I, III and IV of ETC [22]. Furthermore, experiments on isolated porcine heart mitochondria demonstrated that Ca2+ directly stimulates ATP synthase (complex V), enhancing respiratory chain activity and increasing ATP production [23].
However, intense ETC activity leads to increased production of mitoROS, which can overwhelm cellular antioxidant defenses, causing harmful damage, particularly during I/R when mitochondrial Ca2+ overload correlates with a significant increase of ROS and oxidative stress [24].
As anticipated above, RyR2 is a Ca2+ channel that can be found also in close proximity to MAMs to guarantee the correct release of Ca2+ towards mitochondria. Functional anomalies in RyR2 Ca2+ release have a noteworthy symptomatic impact in cardiac disease [9]; in a post-MI murine model, sustained Ca2+ leakage through RyR2 from SR leads to mitochondrial Ca2+ overload and a consequent mitoROS production, which cause oxidation of the receptor and an aberrant Ca2+ leak, creating a feedback loop [25]. RyR2 contain multiple cysteine residues, making them susceptible to oxidative changes. Their sensitivity to redox alterations means that the effects of ROS on RyR2 can vary based on concentration. Low levels of oxidants can boost RyR2 activity, while persistent high levels lead to irreversible inhibition, possibly affecting individual cysteine residues differently. Various oxidative modifications like S-glutathionylation and S-nitrosylation impact RyR2 function [23]. Additionally, oxidative stress can activate RyR2 by promoting disulfide bond formation between subunits, altering the channel’s structure and reducing SR Ca2+. Modulation of mitochondrial Ca2+ levels could be regulated also by RyR2 because, upon activation, RyR2 releases Ca2+ ions into the cytoplasm, which can subsequently enter the mitochondria through MCU [24]. This suggests that modulation of RyR2 function may have a protective effect against mitochondrial Ca2+ overload that occurs during IRI. Further evidence showed that RyR2 oxidation increases channel activity and worsens defective intracellular Ca2+ homeostasis [25].
In a time course manner after AMI, RyR2 expression was monitored with the recording of a transient decrease, followed by an increase only during the 4-week recovery, suggesting a role of this channel in the compensatory reaction of rat cardiac tissue to injury [26]. Of note, during I/R RyR2 is reported to be phosphorylated by Ca2+/calmodulin-dependent protein kinase II (CaMKII) at S2814; this site of phosphorylation is crucial for the cardiac damage probably linked to the increase in SR Ca2+ leak and consequent mitochondrial Ca2+ overload. Knock-in mice carrying a genetically inactivated site on RyR2 revealed a strongly reduced necrosis and apoptosis, thus a protection from I/R injury (IRI). By contrary, knock-in mice with the constitutively activated form of the aminoacidic site, presented a much more severe phenotype [27]. Accordingly, several studies demonstrated that ablation of CaMKIIδ, the main isoform in the myocardium, protects against I/R, suggesting a promising target for heart protection [28, 29].
Aberrations of other SR Ca2+ handling proteins are associated with AMI, such as SERCA2a. This pump is essential in controlling systole and diastole events as it modulates the cytosolic Ca2+ and thus the amount of Ca2+ bound to Troponin C. During I/R, there is an impairment of the normal influx of Ca2+ resulting in an overload of the amount of intracellular Ca2+ and a decrease in the activity of the SERCA2a isoform [30, 31]. Several studies over the years have demonstrated that increased SERCA2a expression can improve myocardial contractility and Ca2+ management following I/R myocardial injury [32, 33]. Of note, SERCA2a affinity for Ca2+ is carefully modulated by the interaction with phospholamban (PLB), whose expression levels and the phosphorylation status may limit or allow Ca2+ reuptake into the SR. This mechanism is regulated either by protein kinase A (PKA) or by CaMK, both proteins can phosphorylate PLB, releasing its inhibitory effects on SERCA2a [34]. A study by Shintani-Ishida demonstrated a significant PLB dephosphorylation associated to ischemic episodes in an in vivo model of AMI, that allows to cytosolic Ca2+ overload in early reperfusion, contributing to the formation of contraction bands [35].
The contractile dysfunction encountered following I/R and widely described until now can be further ascribed to the proteolytic modification of SR proteins like Junctophilins (JPH) 1 and 2 [36], calcineurin, protein kinase C (PKC), SERCA2a. This happens following the activation of Ca2+-dependent proteases, such as calpains, during Ca2+ overload that occurs in I/R [37]. Indeed, both JPH1 and JPH2 proteins are recognized as target of calpain-1 and 2, whose activity enhances during stress conditions [38]. Their expression, in particularly of JPH2, is downregulated during IRI [38].
Of note, in I/R, mitochondria are the first sensing organelles of the lower presence of oxygen; the ETC activity is inhibited and a consequent significant depletion in ATP production occurs. In this condition the cell favorizes a metabolic switch to anaerobic glycolysis. This leads to an intracellular Na+ and Ca2+ overload as a compensatory mechanism to buffer the excessive H+, mediated respectively by the activation of the Na+/H+ exchanger [39], inhibition of Na+/ Ca2+ antiporter (NCX) [40, 41]. Intracellular Ca2+ levels and membrane depolarization can also regulate the activity of large-conductance calcium-activated potassium ion channels (BKCa channels). These channels participate in a wide variety of fundamental physiological processes from vascular tone and cardiac rhythmicity [42]. BKCa channels have been detected in the IMM of adult cardiomyocytes where they increases K+conductance and improves mitochondria respiratory function by reducing the production of mitoROS and decreasing deleterious intra-mitochondrial Ca2+ accumulation occurring after I/R injury [43,44,45]. Increased production of mitoROS especially during cardiac reperfusion triggers the opening of another channel: the mitochondrial permeability transition pore (mPTP) [40, 41]. Opening of the mPTP is characterized by depolarization of the ΨMand from to exposure to high levels of mitoROS. During AMI, oxygen deprivation impairs oxidative phosphorylation, causing ion dysregulation. During reperfusion, the oxygen-starved heart undergoes oxidative damage due to the sudden abundance of nutrients and O2, triggering mPTP-dependent cell death [46, 47]. The intricate relationship between malfunctioning mitochondria and disrupted Ca2+ regulation underscores the intricacy of cardiomyocyte death during myocardial reperfusion injury. Key contributors to cell death in this context include hypercontracture and mitochondrial permeability transition (MPT), both exacerbated by incomplete repolarization of mitochondrial membranes. Hypercontracture arises from excessive contractile activity promoted by restored energy production in presence of elevated cytosolic Ca2+ levels. However, in tissues, the mechanical strain stemming from neighboring cell hypercontraction leads to mutual cellular breakdown and necrosis [48].
Whether the MCU-mediated Ca2+ influx is confirmed to be an important regulator of cardiac metabolism (i.e., ATP production) and in heart contractility in response to mechanisms of mild stress, its role in I/R remains controversial, at least from the analysis of data presented in the literature. In 2015, the groups of Elrod JW and Molkentin JD, independently showed how the inducible and conditional loss of cardiac MCU in a mouse model of I/R limits mitochondrial Ca2+ overload, the irreversible opening of mPTP and thus cell death; as consequence, the hearts resulted to be protected from bigger IS in reperfusion [24, 49]. By contrary, by taking advantage from a mouse model carrying a total deletion of MCU, Finkel’s group revealed the absence of IRI prevention. Hearts from WT and MCU−/− mice had the same levels of apoptosis, cell contracture and no differences in mPTP opening [50]. However, although MCU depletion limited mitochondrial Ca2+ uptake also in this animal model, the basal metabolism remained unchanged. It cannot be hidden that data reported until now are controversial. Different results might be explained by the mouse model studied: whether MCU is deleted in the whole body, the onset of some compensation mechanisms might interfere with the physio pathological readout; currently, the inducible and conditional loss of cardiac MCU can be the most reliable method to assess mitochondrial Ca2+ role during ischemia.
A very recent work by Ashok et al., demonstrated that mitochondrial NCX is the primary way of Ca2+ entry in mitochondria of neonatal mouse ventricular myocyte knock-out for MCU [51]. This work supports the hypothesis of the adaptation of the mouse model carrying a germline deletion of MCU, in which Ca2+ entry in mitochondria might be controlled in different ways.
More recently, without the use of transgenic preclinical models Guan L and colleagues reported a significant upregulation of MCU in IRI, confirming that the resulting mitochondrial Ca2+ overload led to dysregulation at multiple levels including the imbalance of mitochondrial quality control mechanisms like fusion, fission and mitophagy and the activation of calpains [52].
MCU is not the only one pore-forming protein of the complex. Also, MCUb plays crucial roles in Ca2+ channeling and it is considered as the dominant negative subunit of MCU [53]. To confirm in alternative ways the role of mitochondrial Ca2+ in I/R, in 2020 Molkentin JD and colleagues replicated the study carried out in 2015 to understand the behavior of this subunit under I/R conditions [54]. He described a significant upregulation of MCUb starting from 3 days after ischemia without detecting the protein at resting state or early at reperfusion time [54]. Although this could mean that MCUb adaptations can have protective roles during later stages of reperfusion, the exact ratio among MCU – MCUb – EMRE and its significance should be carefully evaluated under these experimental conditions.
Ca2+ dysregulation at MAMs in myocardial infarctionMAMs are specialized regions where mitochondria and the SR come close together. Recent advancements in biomedical techniques have allowed a better visualization of this compartment in living cells using fluorescence confocal microscopy. MAMs act as biochemically independent areas while serving as communication points between SR and mitochondria, maximizing their signaling interactions. As we previously highlighted the importance of SR and mitochondria in AMI, it’s worth noting that MAMs also play a crucial role in this context. Indeed, they constitute several microdomains with high Ca2+ concentrations, thus being essential for cardiomyocytes in regulating Ca2+ transfer to mitochondria and supporting energy production. Thanks to the use of electron tomography, it has been demonstrated that SR and mitochondria are connected by tethers with a distance of approximately 10–30 nm and it has been defined a fundamental reliance of cell function and viability on the preservation of appropriate spacing between the SR and mitochondria [55].
Evidence suggests that dysfunctions at MAMs may contribute to the pathogenesis of reperfusion injury following AMI, suggesting that a decrease in the tethering between the two organelles is associated with a disturbance of clearance and ER stress, and a decline of mitochondrial dynamics included mitochondrial Ca2+ uptake, which, in turn, contributes to a decrease in cell death in cardiac myocytes subjected to I/R [56].
From a historical point of view, the first protein complex identified at MAMs was the IP3Rs/GRP75/VDAC1 axis. The different isoforms of the ER membrane IP3R are linked to voltage-dependent anion channel 1 (VDAC1) localized at OMM by glucose-regulated protein 75 chaperone (GRP75). This complex plays a critical role in enabling Ca2+ transfer between the two organelles, consequently controlling either the apoptotic process or the energy production. Specifically, IP3R3-GRP75-VDAC1 complex is implicated in mitochondrial Ca2+ overload and subsequent cardiomyocyte death observed during the reperfusion phase after sustained ischemic insult. Furthermore, the mitochondrial matrix protein Cyclophilin D (CypD) is also known as a regulator of mPTP activity [46], can interact with IP3R1-GRP75-VDAC1 complex. This interaction acts to regulate Ca2+ exchange from SR to mitochondria (Fig. 1) [57]. Proofs highlighting the relevance of VDAC1 in this pathological context come from a study carried out on a rat model of MI and on human cardiac tissues obtained from post-MI patients. The findings from these investigations unveiled the upregulation of VDAC1 levels; when inhibited through the oligomerization inhibitor VBIT-4 it relieves the increased fibrosis in the atrial myocardium of rats subjected to MI [58]. Further investigations have focused on glycogen synthase kinase-3β (GSK3β), which in its active form can phosphorylate VDAC1 and increase mitochondrial Ca2+ uptake. Moreover it has been revealed that in perfused rat hearts treated with GSK inhibitors, the ischemic process is less harmful on heart function [59, 60].
FUN14 domain containing 1 (FUNDC1) is a highly conserved OMM protein which plays a crucial role at MAMs: it is activated under ischemic conditions to induce mitophagy; while after reperfusion it is phosphorylated and inactivated resulting in reduction of mitophagy and activation of apoptosis [61]. FUNDC1 interacts with IP3R2 to control ER Ca2+ release into mitochondria; indeed, when depleted it leads to disruption of MAMs and to mitochondrial dysfunction [62]. Cardiomyocyte-conditional deletion of FUNDC1 provokes heart failure in vivo, which is worsened by acute MI: at molecular level this is explained by the disruption of MAMs integrity, showed as a decrease of MAMs proteins expression and a dissociation between mitochondria and ER, and a consequent impairment in Ca2+ homeostasis [62]. Other evidence both in vitro and in vivo confirmed the significance of FUNDC1 in myocardial injury following ischemic events, its expression and the mitophagic control are repressed leading to mitochondrial impairments and cardiomyocyte apoptotic death [63].
A key protein is also represented by Mitofusin 2 (MFN2), usually involved in controlling mitochondrial fusion, it is localized at ER and OMM interface and through the formation of homo- or hetero-dimers with MFN1 or MFN2 promotes MAMs stabilization (Fig. 1). Mitofusins revealed to be essential in cardiovascular system as they control mitochondrial fusion and ensure the correct mitochondrial morphology necessary for cardiac respiration and contraction [64].
MFN2 exhibits contrasting roles in MI and myocardial IRI. Some evidence suggests that MFN1/MFN2 double-knockout mice died at the embryonic stage due to lethal cardiac damage and conditional deletion in adult mouse hearts leads to severe impairments in mitochondrial functionality and cardiac respiration. Despite that, hearts deficient in both MFN1 and MFN2 are protected against acute IRI, due to an increased resistance to mPTP opening in response to Ca2+ and a reduction in mitochondria–SR interaction, suggesting that hearts deleted of both proteins are resistant to AMI [65]. Notably, MFN2-deficient hearts showed a less severe phenotype compared to double MFNs
留言 (0)