
記住我
The CREW-I study (Cardiac REperfusion With Intralipid at reperfusion study) was an academic, monocentric, prospective, randomized, double-blind, pilot trial conducted at the Groote Schuur Hospital in Cape Town, South Africa. The trial was authorized by the Human Research Ethics Council (HREC) of the University of Cape Town (number: 806/2014) and by the Medicines Control Council (MCC) of South Africa (number: 20150807). The trial was registered in ClinicalTrials.gov before the start of the study (registration number: NCT02807727) on June 16, 2016. The trial was conducted according to the requirements of the Declaration of Helsinki. Written informed consent was obtained from all participants.
PatientsConsecutive patients scheduled for first time elective isolated CABG on CPB were screened for eligibility. Patients were eligible for inclusion if they were aged between 18 and 65 years, had left ventricular ejection fraction greater than 40% and body mass index between 21 and 35 kg/m2. Exclusion criteria were diabetes mellitus, creatinine > 200 μmol/l, myocardial infarction within the previous 2 weeks, inotropic support prior to surgery, contraindications to Intralipid (including previous hypertriglyceridemia pancreatitis, plasma triglyceride levels > 5.7 mmol/l, egg, peanut, and soybean allergy), treatment with Glibenclamide or Nicorandil (which may interfere with cardioprotection) [15], and participation in another interventional trial within 30 days.
Peri-operative ProcedureThe decision to maintain chronic treatments (e.g., statins, beta-blockers, etc.) prior to surgery was left to the discretion of the physicians in charge and followed international guidelines. Surgery for this study was performed by two experienced surgeons using a similar technique regarding bypass management, cardioplegia, and selection of grafts; they were blinded to the treatment allocation. Induction of anesthesia consisted of intravenous sufentanil (1 µg/kg), etomidate (0.2 mg/kg), rocuronium (0.6 mg/kg). Anesthesia was maintained with isoflurane (0.6–1.8%). After median sternotomy and systemic heparinization, the ascending aorta and right atrium and were cannulated to establish CPB. After cross clamping, arrest was achieved with blood-based St. Thomas’ Hospital cardioplegic solution at mild hypothermia (34 °C). After surgery, patients were transferred to intensive care unit (ICU) and extubated at the earliest clinically appropriate time.
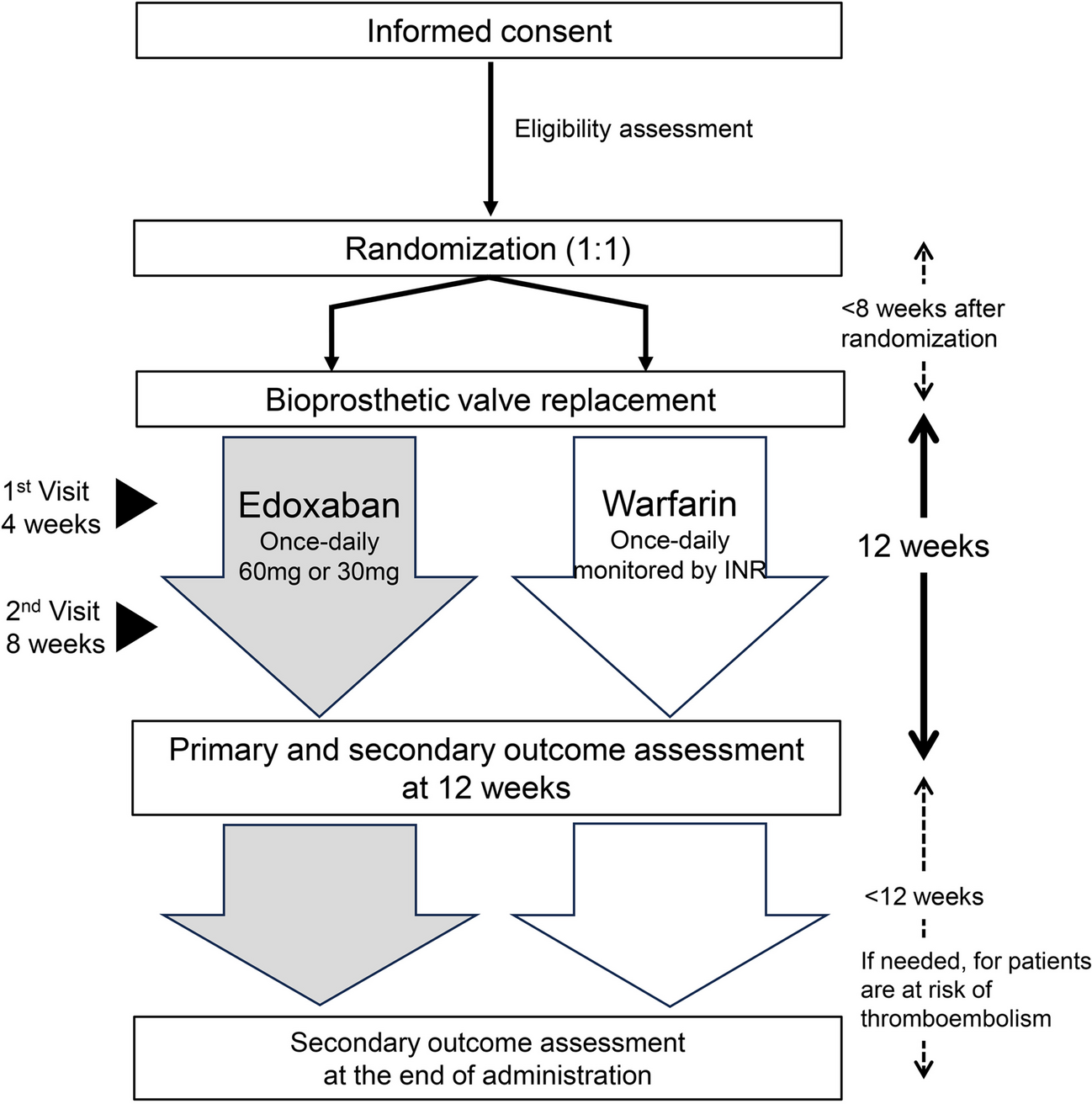
Experimental ProtocolThe experimental protocol is summarized in Fig. 1. Patients who met the enrollment criteria were randomized on a 1:1 basis to either control or Intralipid group using a table of random numbers generated by the study statistician. A pre-compiled study folder was assigned to each patient. The folder had a sequential randomization number together with a barcode generated by a software package (R Studio, Inc. Austria). The barcoded adhesive stickers were used for all study-related investigational procedures, including patient allocation for the issue of study drug, blood samples for analysis, and tissues for storage.
Fig. 1
Experimental protocol of the study. MLR: Modified Lactate’s Ringer; ICU: intensive care unit
Three minutes prior to aortic unclamping (i.e., before myocardial reperfusion), patients received, via central venous catheter, either a rapid infusion of 1.5 ml/kg Intralipid 20% (Fresenius-Kabi, Port Elizabeth, South Africa) for the Intralipid group or 1.5 ml/kg of modified Ringer’s Lactate (Fresenius-Kabi, Port Elizabeth, South Africa) for the Control group, using a concealed administration set and opaque syringe. The dose of Intralipid and timing for administration of the drug was extrapolated from experimental data that showed potent protection [5]; we also considered the pharmacokinetic effect of the CBP circuit. The study duration was limited to the hospital length of stay.
OutcomesThe primary outcome was the mean geometric area under the 72-h curve (AUC) for cardiac troponin I (cTnI) release.
Secondary outcomes included the 72-h AUC of creatine kinase-myocardial band (CK-MB), need for defibrillation, time to extubation, length of ICU and hospital stay, and serious adverse events occurring during hospitalization (death and any peri- and post-intervention complications).
Echocardiography and Biochemical AnalysesLeft ventricular ejection fraction (LVEF) was assessed in patients before inclusion by means of ventriculography. LEVF was also assessed after induction of anesthesia using transesophageal echo.
Post-enrolment, a lipid profile including plasma levels of triglycerides, total-cholesterol, low-density lipoprotein (LDL), and high-density lipoprotein (HDL) cholesterol was obtained for each patient.
Blood samples for the analysis of cTnI and CK-MB were drawn after induction of anesthesia and 1, 6, 9, 12, 24, 48, and 72 h after unclamping the aorta. C-reactive protein (CRP) was measured at 24 h after surgery to assess a potential effect of Intralipid on inflammation.
Statistical AnalysisBased on experimental studies on Intralipid-induced cardioprotection [4,5,6,7] and a clinical trial on remote ischemic conditioning in patients undergoing CABG [16], we expected a 40% reduction of the 72 h AUC of cTnI with Intralipid. Considering a statistical power of 90% and an alfa of 0.05 (two-tailed test), the estimated number of patients per group was 15 after adjustment for withdrawals.
Continuous data are presented as median and 1st and 3rd interquartile or mean ± SEM, according to the distribution of the values. Categorial data are presented as number (percentage). Continuous variables were compared using the Wilcoxon rank-sum test or the Student’s t test, and the Chi-squared, or the Fisher exact test was used for proportions.
The primary endpoint was assessed by the geometric mean difference of the AUC for the cTnI concentration in serum over 72 h (sampled at 1, 6, 12, 24, 48, and 72 h), calculated according to the trapezoid rule, and compared using an unpaired t-test. The same method was used to compare the AUC for CK-MB. Repeated measures of cTnI and CK-MB were also compared using two-way ANOVA (group, time).
Statistical analyses were performed using GraphPad Prism 9 (version 9.4.1, La Jolla, USA). A 2-sided P value of 0.05 or less was considered statistically significant.
留言 (0)