Trial design and participants
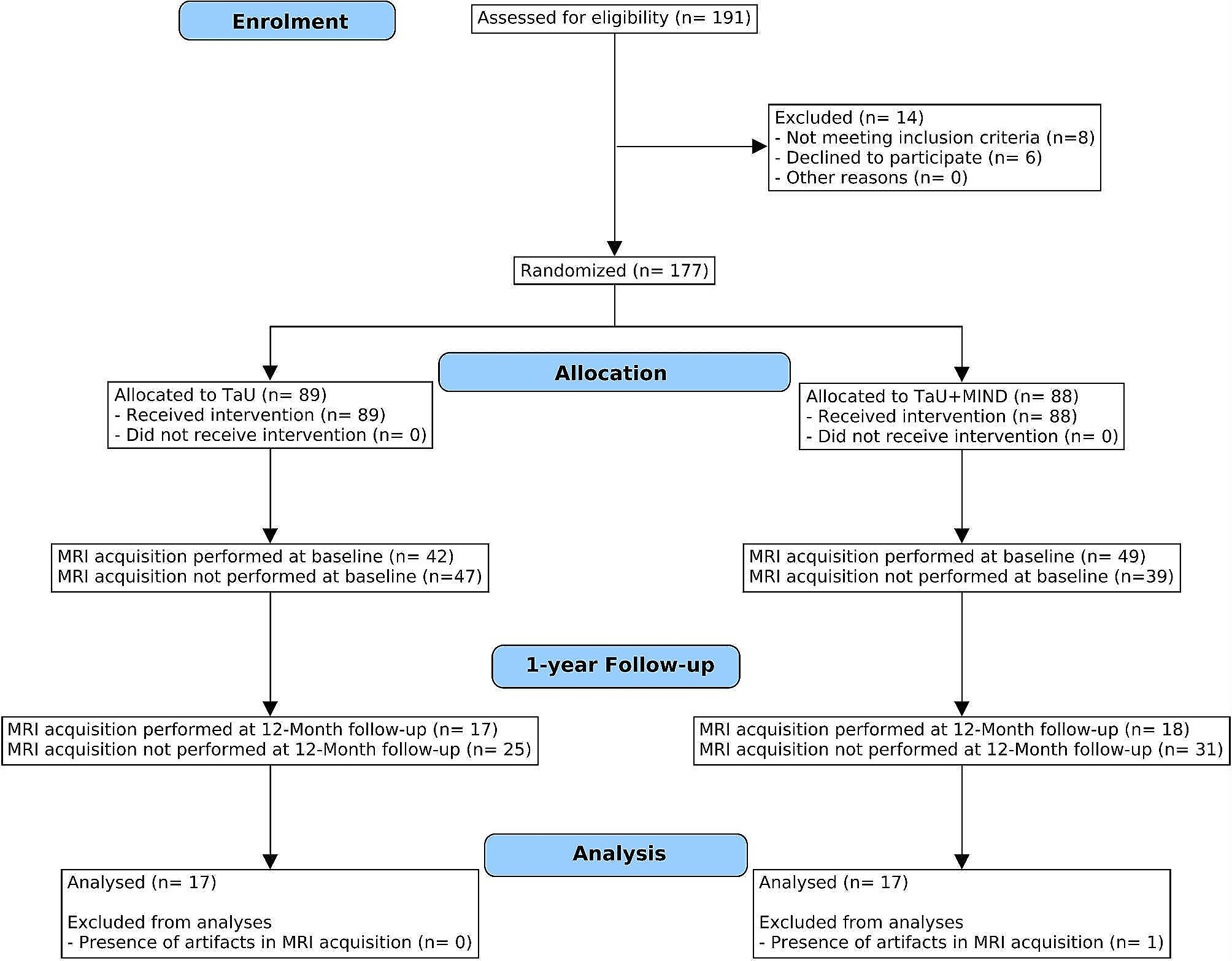
MIND-CM study is a phase-III single-blind Randomized Controlled Trial including CM-MOH patients attending our specialty headache centre for a structured withdrawal treatment. The study was reported in accordance with the CONSORT guidelines [27], and registered on clinicaltrials.gov (NCT03671681). The study started in November 2018; the last patient was enrolled in December 2021; the last follow-up was completed in November 2022.
Inclusion criteria consisted of diagnosis of CM-MOH (codes 1.3 and 8.2) according to the Headache Classification Committee of the International Headache Society guidelines, 3rd edition [2]. Patients with neurological and severe psychiatric comorbidities, pregnancy, other-than-MOH secondary headaches, withdrawal from Medication Overuse Headache twice or more in the last two years, and any previous experience with mindfulness practice were excluded.
All participants gave their written consent. The study was approved by the Ethical Committee of the Fondazione IRCCS Istituto Neurologico “Carlo Besta”, Milan (approval no. 51/2018).
Interventions
The detailed description of the clinical protocol is reported in Grazzi et al. [11].
TaU protocol
The TaU protocol involved withdrawing overused symptomatic medications, tailored prophylaxis, and education on how to correctly use acute medications and how to maintain a healthy lifestyle (e.g., adequate sleep/wake patterns, healthy eating and hydration, physical activity, avoidance of headache triggers) [28]. Prescribed preventive compounds were primarily either neuromodulators (e.g., topiramate or valproate) or antidepressants (e.g., tricyclics or SSRIs). Based on each patient’s clinical profile assessment, other compounds were prescribed when necessary (e.g., beta-blockers).
TaU + MIND protocol
TaU + MIND protocol included TaU with the add-on of six guided sessions of Mindfulness-based intervention. During mindfulness practice, patients focused on the present moment, concentrated on their breath, scanned their body, and paid attention to their bodily sensations [11]. The TaU + MIND program consisted of six 90-minute-long weekly sessions administrated by an expert trained neurologist (L.G.). Within each session, the duration of the mindfulness practice progressively increased from 5 min in the first session to 25 min at the end of the intervention. From the third session onwards, patients were also familiarized with practicing at home with a short session that focused just on breathing. Moreover, patients were instructed to regularly perform 7–10 min of daily home self-practice guided by a 12-minute audio file.
Clinical and neuroimaging assessment
Patients underwent a clinical evaluation at two timepoints: a baseline visit at enrolment (T0) and a follow-up visit after 12 months (T1).
In the clinical assessment, the frequency of headache attacks and symptomatic medications intake (triptan and non-steroidal anti-inflammatory drugs) in the last three months were collected. Moreover, the following tests were administered: Beck Depression Inventory-II (BDI) for depression symptoms [29], State-Trait Anxiety Inventory (STAI-Y) for state and trait anxiety [30], Allodynia Symptoms Checklist (ASC-12) for cutaneous allodynia [31], and Mindful Attention and Awareness Scale (MAAS) for self-awareness [32].
An MRI scan was performed both at T0 and at T1.
Outcomes
The primary outcome of the MIND-CM study consisted of 50% or more headache frequency reduction, in the last 3 months, assessed at 12 months and was previously reported by Grazzi et al. [11] along with other secondary outcomes, as reported in the registered Randomized Controlled Trial protocol.
The registered MRI outcome consists of changes in neuroimaging patterns specific to TaU + MIND patients treated with mindfulness added to prescribed therapy with neuromodulators or antidepressants with respect to the TaU group. Unfortunately, the COVID-19 pandemic interfered with our Randomized Controlled Trial, therefore several patients could not perform the follow-up assessment at our institute due to mobility restrictions. Hence, it was not possible to test the effects associated with prophylaxis (i.e., neuromodulators vs. antidepressants) on functional connectivity amongst TaU + MIND and TaU patients. Therefore, the expected outcome of our study is a change in the functional connectivity of TaU + MIND patients irrespective of the pharmacological prophylaxis.
Sample size calculation
Based on sample size computation, randomization was estimated to involve 170 patients [11]. This calculation was based on the hypothesis that 48% of TaU patients would achieve ≥ 50% headache-day reduction after one year, and that mindfulness practice add-on would increase this figure by 20%. At least 75 patients per group (TaU + MIND and TaU) were considered necessary with alpha set at 0.05 and power at 80%, with an estimate of 12% drop-out at follow-up.
Randomization
Patients were randomly assigned to TaU and TaU + MIND in a 1:1 ratio, using a computer-generated list (simple randomization). The enrolling and evaluating neurologist (D.D.) remained blind to the allocation; A.R. prepared the randomization list and a set of opaque envelopes, randomized patients and handled data collection with other researchers; mindfulness sessions were conducted by L.G.
After screening, eligible patients voluntarily joined the study by signing the informed consent, ensuring they understood the purpose and the blinded evaluation by the neurologist (D.D.). Patients were reminded not to disclose their group allocation. A subsample of ~ 60 patients was expected to undergo MRI acquisition both at the baseline (T0) and at the follow-up (T1), in order to split the sample into 15 TaU + MIND patients treated with antidepressants, 15 TaU + MIND patients treated with neuromodulators, 15 TaU patients treated with antidepressants, and 15 TaU patients treated with neuromodulators. No sample size calculation was performed at this stage to determine the number of participants necessary for MRI sessions.
MRI acquisition
MRI acquisitions were performed at the Department of Neuroradiology, Fondazione IRCCS Istituto Neurologico “Carlo Besta”, Milan (Italy), on a 3T scanner (Achieva dStream, Philips Healthcare BV, Best, NL) using a 32-channel head coil. All MRI images were visually inspected by an experienced neuroradiologist (A.E.).
At each timepoint (T0 and T1), a functional rs-fMRI sequence (eyes opened; T2*-weighted BOLD echo-planar imaging gradient-echo sequence; Repetition Time [TR] = 2000ms; Echo Time [TE] = 30ms; Field-of-View [FOV] = 80 × 80mm; voxel size = 3 × 3 × 3.2mm3; interslice gap = 0.4 mm; flip angle = 80°; 34 axial slices; 450 volumes; Phase Encoding direction = posterior/anterior; acquisition duration = 15 min), a high-resolution structural 3D T1-weighted image (TR = 8.11s; TE = 3.71ms; FOV = 240 × 240mm; voxel size = 1 × 1 × 1mm3; flip angle = 8°; 185 sagittal slices), and a 3D FLAIR sequence (TR = 5000ms; TE = 30ms; inversion time = 1700ms; FOV = 240 × 240mm; voxel size = 1 × 1 × 1mm3; flip angle = 90°; 180 axial slices) were acquired.
The quality of structural and functional images was assessed and visually inspected using the BIDS-compliant software MRIQC [33].
MRI pre-processing
Connectivity analyses were performed using CONN connectivity toolbox (v. 20.b; running in Matlab 2020b) [34] with the “default_MNI” preprocessing and denoising pipeline (smoothing = 6 mm3, aCompCor denoising, 0.008–0.1 Hz bandpass filter). T1-weighted and FLAIR images were bias field corrected and cortical surfaces were reconstructed with the “recon-all” pipeline as implemented in FreeSurfer (version 7; https://surfer.nmr.mgh.harvard.edu/); smoothing = 15 mm3. FreeSurfer longitudinal pipeline was run for each patient [35].
Statistical analyses
Statistical analyses were conducted to: (i) assess differences in demographic and clinical variables between groups at T0; (ii) investigate treatment-related longitudinal differences in clinical variables between groups; (iii) assess distinct longitudinal changes of SN, DMN, and FPN seed-based resting state functional connectivity between groups; (iv) estimate correlations between connectivity changes and improvements in clinical variables; and (v) assess longitudinal structural whole-brain changes between groups.
Demographic and clinical data analyses
Normality test was performed for all variables using Shapiro-Wilk test. The following variables were assessed only at T0 and compared between groups (i.e., TaU + MIND and TaU) using the U Mann-Whitney or the χ2 test: age (in years), sex assigned at birth, years of formal education, years of migraine duration (i.e., age at T0 minus reported age at migraine onset), years of chronic migraine duration, type of overused medications, and prophylaxis assigned as treatment.
To determine differences between groups in clinical variables at T0 (frequency of headache attacks, medication intake, depression severity, state and trait anxiety, allodynia, and self-awareness score), the U Mann-Whitney test was used.
Moreover, longitudinal differences in clinical variables within groups (TaU + MIND T1 vs. T0; TaU T1 vs. T0) were assessed using Wilcoxon signed-rank test.
Finally, to investigate treatment-related longitudinal differences (Δ = T1 – T0) in clinical variables between groups, changes between T1 and T0 (Δ TaU + MIND vs. Δ TaU) in the same clinical variables were assessed using U Mann-Whitney test.
All between-group comparisons were performed and reported both with and without whole-sample outlier removal using each variable’s mean ± 3 standard deviations as a threshold. A p < 0.05 was considered statistically significant. All analyses were performed with R 4.2.1.
Resting-state fMRI analyses
For each participant at each timepoint, a seed-to-voxel approach was used to estimate the whole-brain connectivity of DMN (medial prefrontal cortex, bilateral lateral parietal region, posterior cingulate cortex), SN (anterior cingulate cortex, bilateral anterior insula, bilateral rostral prefrontal cortex, bilateral supramarginal gyrus), and FPN (bilateral lateral prefrontal cortex, bilateral posterior parietal cortex) using the available pre-defined regions in the networks atlas as implemented in CONN [34]. For each rs-fMRI network, Pearson’s correlation coefficients were computed between the average of signal time-series of each region of interest and all brain voxels. Correlation coefficients were then converted to Z scores with the R-to-Z Fisher transform. Connectivity maps of each network (DMN, SN, and FPN) were entered into a separate second-level general linear model to assess functional connectivity differences in network profiles between TaU + MIND and TaU patients. Between-group functional connectivity differences were assessed at the baseline (TaU + MIND T0 vs. TaU T0) and at the follow-up (Δ TaU + MIND vs. Δ TaU). Age and sex assigned at birth were included as nuisance covariates. All results were FWE corrected at p < 0.05 at the cluster level and p < 0.001 uncorrected at the voxel level (i.e., a p < 0.001 cluster-defining primary threshold was applied to all voxels, then FWE correction was applied to the resulting clusters to correct p-values for multiple comparisons to avoid false-positive findings). Finally, for all significant results, effect size (Cohen’s d) was estimated. A Cohen’s d > 0.5 was considered as indicative of a large effect.
Correlational analyses
To estimate correlations between functional connectivity changes and improvements in clinical variables, connectivity values from significant clusters resulting from rs-fMRI longitudinal between-group comparisons (Δ TaU + MIND vs. Δ TaU) were extracted. Normality of variables was tested with Shapiro-Wilk test. Then, connectivity values were correlated to corresponding variations in clinical variables (Δ) using Pearson’s correlations (r) separately for each group.
Structural analyses
Two separate structural analyses were performed to assess whether the functional connectivity changes were accompanied by co-occurring morphological variations: a region of interest-based analysis and a whole-brain analysis.
For statistically significant functional connectivity clusters obtained in rs-fMRI longitudinal between-group comparisons (Δ TaU + MIND vs. Δ TaU), a region of interest-based analysis was applied. Mean cortical thickness values were extracted from significant functional clusters with FreeSurfer in each patient at each timepoint. Then, longitudinal between-group comparisons were performed using U-Mann-Whitney test (Δ TaU + MIND vs. Δ TaU).
To evaluate structural alterations across the entire brain between the TaU + MIND and TaU groups at baseline and longitudinally, a whole-brain analysis was performed. A general linear model was fitted using FreeSurfer vertex-wise analyses to ensure that no between-group differences in whole brain cortical thickness were present at T0 (TaU + MIND T0 vs. TaU T0). Finally, FreeSurfer longitudinal pipeline was adopted to compare vertex-wise longitudinal changes between TaU + MIND and TaU groups (Δ TaU + MIND vs. Δ TaU). In vertex-wise analysis, age was considered as a covariate. All results were corrected for multiple comparisons and considered significant if surviving a p < 0.001 vertex-wise threshold and a p-FWE < 0.05 cluster-wise threshold. For all significant results, effect size (Cohen’s d) was estimated.







留言 (0)