
記住我


Overall, 124 neonates presenting with distal intestinal obstruction (and with a patent anus) were identified and all were included. Of these, 86 (69%) were males. The median gestational age was thirty-nine weeks (IQR 38–40 weeks) with a median birth weight of 3330 g (IQR 3055–3660 g). Median age at presentation was 2 days (IQR 1–3 days).
Five (4%) of these neonates had bowel pathology suspected antenatally with findings of both echogenic and dilated bowel (n = 2), dilated bowel alone (n = 1), and echogenic bowel in isolation (n = 1). Initial symptoms and signs of the 124 neonates included vomiting at presentation in 107 (86%) which was bilious from the outset in 74, became bilious in eight and was always non-bilious in the remainder. Seventeen (14%) neonates did not present with vomiting. One hundred and eighteen (95%) neonates had abdominal distension at presentation and 93 (75%) had delayed passage of meconium. Seventy (56%) neonates presented with all three symptoms of vomiting, abdominal distension, and delayed passage of meconium. One neonate was additionally felt to have symptoms and signs of enterocolitis.
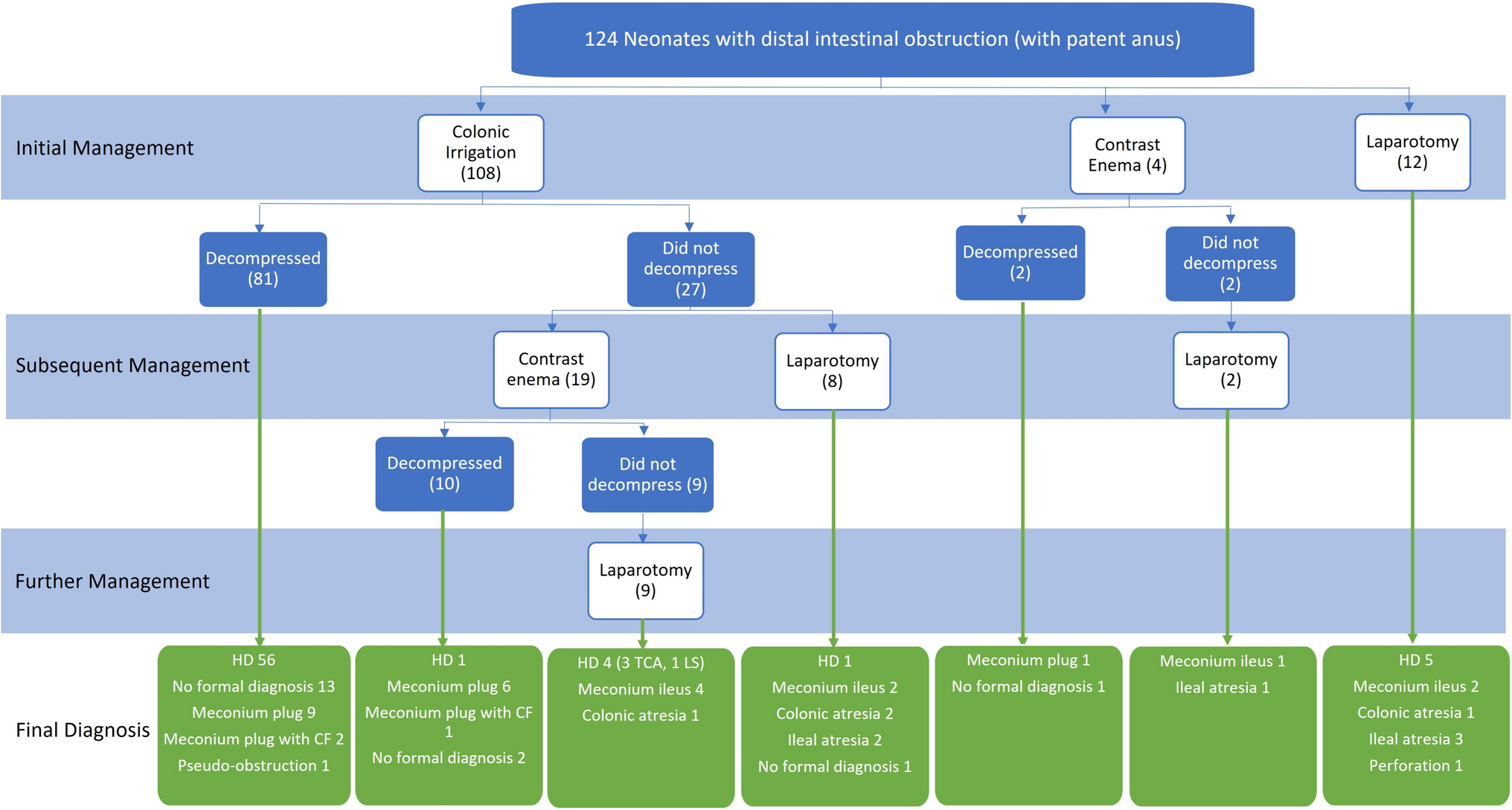
InterventionsDetails of initial and subsequent interventions and final outcome are shown in Fig. 1.
Fig. 1
Management and final diagnosis. HD Hirschsprung disease; CF cystic fibrosis; TCA total colonic aganglionosis; LS long segment
The most frequent initial intervention was colonic irrigations which were performed in 108 (87%) neonates. Decompression was achieved in 81 (75%). Subsequent management in the 27 (25%) neonates in whom irrigations did not achieve decompression was contrast enema in 19 (70%) and laparotomy in 8. Of those having contrast enema after failed colonic irrigations, decompression was achieved in 37% (n = 10) with the remainder proceeding to laparotomy. Of those who decompressed with irrigations alone, four subsequently re-obstructed requiring surgery. All four had a final diagnosis of Hirschsprung disease although this was not known at time of surgery.
Overall, twelve (10%) neonates had an initial laparotomy. In 5 of these the indication was evidence of intestinal perforation on their abdominal radiograph, in 2 due to clinical signs of an acute abdomen and in 3 the combination of distal bowel obstruction and antenatal bowel dilatation that was suggestive of a cause requiring surgical intervention. A further 19 had a laparotomy to achieve decompression of the gastrointestinal tract following unsuccessful attempts via irrigations or contrast enema. In the 5 who underwent laparotomy on the basis of suspected perforation, findings were caecal perforation and subsequent diagnosis of Hirschsprung disease in 3, colonic atresia with perforation in 1 and terminal ileal atresia with perforation in 1.
Additional investigationsOverall, 106 (86%) neonates had SRB taken during their initial admission. Sixty-six (62%) of these resulted in a diagnosis of Hirschsprung disease.
All but two of the 81 neonates who achieved decompression with irrigations alone had SRB. One neonate was diagnosed with meconium plug and cystic fibrosis therefore decision not to undertake SRB. The other neonate was discharged without having a SRB but was subsequently readmitted with symptoms suggestive of Hirschsprung’s enterocolitis. SRB confirmed the diagnosis of Hirschsprung disease. All of the infants who achieved decompression with contrast enema also had SRB. All but one of the neonates who passed a meconium plug had SRB, 1 did not due to family history of cystic fibrosis therefore only cystic fibrosis testing was performed which was positive.
Overall, 41 neonates were tested for cystic fibrosis, with 12 (35%) positive results. All 9 cases of meconium ileus encountered at laparotomy underwent testing for cystic fibrosis and all were positive. The majority (n = 15/18) of neonates who passed a meconium plug had testing for cystic fibrosis and 3 were positive. Other neonates were tested for cystic fibrosis according to surgeon preference or specific heightened suspicion. Final diagnosis in these other cases tested for cystic fibrosis was ileal atresia (n = 1), Hirschsprung disease (n = 9) no formal diagnosis (n = 7).
Final diagnosis and outcomeThe most common final diagnosis identified in this patient population was Hirschsprung disease affecting 67 (54%) of all neonates admitted with distal intestinal obstruction. Nine (7%) had meconium ileus associated with cystic fibrosis, and 19 (15%) had a discharge diagnosis of meconium plug syndrome (including 3 with cystic fibrosis). There were 10 (8%) neonates with intestinal atresia, (6 ileal, 4 colonic), 1 perforation without underlying aetiology identified, and 1 intestinal pseudo-obstruction. In the remaining 17 cases (14%) no formal underlying cause could be identified. This ‘no formal diagnosis’ was made as a diagnosis of exclusion with most having a SRB that was negative for Hirschsprung disease, there being no suspicion of alternate diagnosis (including some who had cystic fibrosis testing) and had adequate follow-up to be certain they were passing stool normally without concern. Just one infant was erroneously given this diagnosis initially who represented later and was found to have Hirschsprung disease.
None of this group of neonates died during the neonatal period with all surviving to discharge from the neonatal unit. Median length of neonatal stay was 11 days (IQR 7–19 days).
Impact of antenatal diagnosisOf the 5 neonates suspected to have intestinal pathology antenatally, three had meconium ileus, one had ileal atresia and one had meconium plug syndrome. Four had confirmed diagnosis of cystic fibrosis, one had a normal genetic screen. Four of these five neonates required a laparotomy. Thus the combination of antenatal findings and neonatal distal intestinal obstruction resulted in significant pathology in 4 of 5 cases.
Factors associated with final diagnosisOverall distribution of key symptoms and signs at presentation was similar across all final diagnosis groups including in neonates with no underlying cause identified (Fig. 2). All three symptoms/signs—vomiting, abdominal distension and delayed passage of meconium—were present in 55% of cases of Hirschsprung disease, 36% of cases with meconium ileus, 70% of cases of meconium plug syndrome, 43% of cases of ileal atresia, 50% of cases of colonic atresia and 41% of cases with no underlying cause identified. Hence presence or absence of these clinical features was not useful as a predictor of final outcome or as a guide to interventions or investigations. Similarly there was no association between timing of presentation and final diagnosis although all these cases presented in the immediate newborn period.
Fig. 2
Distribution of symptoms and signs at presentation. HD Hirschsprung disease; MI meconium ileus; MP meconium plug syndrome; IA ileal atresia; CA colonic atresia; NFD no formal diagnosis
In the group of neonates who could be decompressed with colonic irrigations the most common diagnosis was Hirschsprung disease (56/81; 69%) followed by no formal diagnosis (13/81; 16%). Amongst neonates undergoing other interventions, Hirschsprung disease was less prevalent (Fig. 1). Conversely most neonates ultimately diagnosed with Hirschsprung disease (56/67; 84%) could be decompressed with irrigations without requiring contrast enema. Just one was decompressed with contrast enema and the remainder required surgical decompression.
Neonates who required contrast enema to achieve decompression were most likely (10/12) to have no significant pathology (meconium plug or no formal diagnosis). All but one infant who underwent laparotomy did have significant pathology including, unsurprisingly, all 10 neonates with a final diagnosis of intestinal atresia.
All sixteen of the neonates with final diagnosis of meconium plug syndrome without cystic fibrosis achieved decompression without a laparotomy. This diagnosis was made based on passage of a meconium plug during either irrigation (n = 9) or contrast enema (n = 7, often with characteristic visualisation of meconium plugs on contrast enema) followed by no re-obstruction and negative tests for both Hirschsprung disease and cystic fibrosis (when performed). Conversely of the 20 neonates who passed a meconium plug, three had cystic fibrosis and just one had Hirschsprung disease.
Ultimately, 17 (14%) neonates had no formal diagnosis made, the majority of whom (16 [94%]) decompressed with colonic irrigation or contrast enema. One neonate who did not compress with irrigations had a persistent abnormal abdominal radiograph and proceeded to exploratory laparotomy at which no abnormality was found. Cystic fibrosis test was negative and a decision not to perform SRB was made unless the baby had further symptoms.
留言 (0)