This research reports the results of post-mortem genetic testing performed through a comprehensive NGS analysis of genes associated with arrhythmogenic syndromes in a cohort of 76 SIDS cases.
As said, although the pathophysiological mechanism underlying SIDS is still unclear, it has been hypothesized that death is due to fatal arrhythmias dependent on the infant’s genetic background [22, 23]. Currently, a genetic cardiac predisposition that may have contributed to arrhythmogenic sudden infant death has been identified in several cohorts. This predisposition consists of rare/ultra-rare variants associated with inherited cardiac conditions (i.e., primary arrhythmia syndromes and structural cardiac diseases) [5, 24,25,26,27,28]. The main difficulties in identifying the actual burden of cardiac genetic predisposition in SIDS by comparing existing studies lie in the different types of post-mortem genetic testing performed, the panel of genes analyzed and the VAF cutoff considered.
In our study, NGS analysis was performed using a custom resequencing panel of selected genes related to SCD. Indeed, there is a well-established consensus that about 10–15% of SIDS are due to pathogenic mutations in cardiac channelopathy-associated genes [5, 9, 29, 30]. Moreover, we also considered genes associated with cardiomyopathies because alterations in structural proteins can be responsible for arrhythmic events even in absence of macro/microscopic changes. In our study, variants with a VAF < 0,1% were considered rare. This not too strict initial cutoff was set up to avoid excluding functional potentially important variants involved in the pathogenesis of SIDS. Although filtering from the beginning with a lower allele frequency (VAF < 0.005%) might be useful to rule out variants that are too frequent in the general population to cause rare diseases, it might miss potentially important variants related to SIDS but too common to be detected with the applied threshold [9, 31, 32]. With our threshold value set, post-mortem genetic analysis detected 50 carriers of at least one rare genetic variant associated with SCD. PM2_Supporting item in the ACGM classification was considered then fulfilled with VAF < 0.004% for cardiomyopathies and < 0.001% for channelopathies. Additionally, there is currently a lack of specific recommendations or guidelines focused on variant interpretation in forensic medicine, which further complicates accurate genetic assessment in forensic contexts [33].
Our post-mortem genetic testing revealed that in 4 out of 76 cases (5.3%) at least one pathogenic (P) or likely pathogenic (LP) variant could be considered as a monogenic cardiac cause responsible for the sudden death of the infant. Indeed, in all these cases, previous forensic examinations including full autopsy, histopathological, toxicological and microbiological analysis were negative/inconclusive.
The variants TTN_ p.(Leu22480*) and TTN_c.32705-1G > A (rs1285884266) were identified in an infant who died without a clear cause of death after full forensic examination. Both affect the TTN for a myofilament with a key role in the transmission of and maintenance of resting tension during cardiac contraction [34, 35]. Pathogenic variants in TTN are primarily linked to DCM. Although approximately 25% of DCM cases are attributed to truncations in the A-band region of TTN [36], mutations in other regions are also observed. For example, among TTN mutations associated with DCM, Chauveau et al. [37] reported 29 nonsense changes (including three in the I-band, and 26 in the A-band), along with 17 frameshift mutations (three in the I-band, 14 in the A-band). Additionally, 18 mutations affected TTN splicing, and seven were missense mutations (three in the Z-line, three in the I-band and one in the M-line). Hence, in the current study, despite the variant (TTN_c.32705-1G > A) not being situated within the A-band region, it’s noteworthy that other regions of the TTN gene are expressed in the cardiac isoform and potentially relevant to DCM, thus subject to evaluation in the variant analysis. Moreover, for variant classification, we consistently consider all exons of TTN. In our report, we specify when an exon exhibits a low Percentage Spliced In (PSI), referencing the information available at https://www.cardiodb.org/titin/titin_transcripts.php. Both these TTN variants found in our study were previously reported in ClinVar database and AutoPVS1 tool assign a PVS1_Very strong under a DCM phenotype. Following ACMG standards, these variants have been classified as LP because are absent or rare in the general population (PM2_Supporting) and undergo loss of function (LOF) through nonsense-mediated decay (NMD) of mRNA (PVS1_Very strong). The carrier also hosted some VUS variants. In the newborn with the two variants in TTN gene, a segregation analysis would be highly recommended to determine the allele distribution that could be the explanation for such a severe phenotype.
The variant in the MYL3 gene, p.(Val156Leu)—rs199474707, CM1412322- was identified in a one-day-old newborn girl. MYL3 encodes for the cardiac isoform of myosin essential light chain (ELC) modulating heart contraction [38]. This variant is observed in 22 out of 146,180 alleles in gnomAD, with a PopMax filtered frequency of 0.001213%. As previously stated, we consider that an extremely rare variant in cardiomyopathies is defined when the PopMax filtered is lower than 0.004%. Thus, PM2_Supporting item in the ACGM classification was considered fulfilled in the current case. Therefore, despite its infrequent occurrence in the general population, it has been detected in several HCM patients (PS4_Supporting). It is located in a protein domain critical for protein function (PM1_Strong) in a context of HCM and its key role is confirmed by in silico tools, predicting a deleterious effect (PP3). Considering all data, it was classified as LP. Several reports identified the same rare variant in patients diagnosed with HCM. A multivariate analysis performed by Wang et al. revealed that people with multiple rare variants in sarcomere genes have a higher risk of SCD [39]. Thus, the phenotype spectrum associated with the variant p.(Val156Leu) can range from an initially macro/microscopically undetectable condition to profibrotic changes that, at an advanced stage, result in an overt left ventricular hypertrophy (LVH) assessed by imaging techniques. Studies in animal models have shown that pathways involved in fibrosis and collagen deposition are activated early, before LVH is detectable at gross or histological examination [11, 40,41,42,43,44]. Thus, as hypothesized by Brion et al. [11], it is possible that the disruption of sarcomeric activity itself in the earliest stages of the disease, may alter intracellular calcium homeostasis exposing the patient to life-threating arrhythmias (LTAs). These mechanisms could be particularly relevant in SIDS, where there is no visible phenotype as in most incipient forms of the disease. However, further studies are needed to ascertain the role of certain cardiac structural proteins in modulating cardiac electrical conduction. On the other hand, this close interaction between ion channels and structural proteins, has already been established for genes coding for proteins with both structural and arrhythmogenic functions (e.g., SCN5A, RYR2, HCN4, AKAP9).
The variant p.(Trp1684Phe) in SCN5A gene was found in a 3-day-old infant who died while sleeping. Abnormalities in the cardiac sodium channel gene (SCN5A) are mainly associated with BrS and LQTS, which are characterized by an inherited susceptibility to ventricular arrhythmias. However, some variants in this gene cause enlargement of cardiac chambers, resulting in DCM. It has been hypothesized that alterations in this sodium channel may disrupt interactions with the cytoskeleton and intercalar disc or, alternatively, alter the amount of intracellular Ca+2 causing impaired contraction and structural deformation [45, 46]. No gross or histopathological changes were observed in our case. This variant does not result in a frameshift mutation. Its protein-level effect is expected to resemble that of a missense variant. As previously mentioned, although variants in SCN5A may be also reported especially in LQTS, in our case, the variant detected in the infant was classified in the context of BrS due to its location within a domain known to be crucial for the proper functioning of the protein and associated with BrS (PM1_Strong). Moreover, this variant was nearly absent in the general population (PM2_Supporting) and reported only once in ClinVar in a patient diagnosed with BrS. The LP significance of this variant was also supported by PP4 criteria, which a patient’s phenotype or family history is highly specific for a disease with a single genetic etiology. The new international guidelines published in 2022 still maintain SCN5A gene as the only gene with a definitive association with Brugada Syndrome. The risk of ventricular arrhythmias in children with BrS is generally low but fever (particularly frequent in early childhood) is the most important precipitating factor [47]. Moreover, the risk of SCD in pediatric BrS patients appears to be inversely related to age [48]. This evidence may support the role of channelopathies in predisposing infants to the fatal arrhythmias as in SIDS, especially when certain circumstances occur.
Our post-mortem genetic analysis identified a variant in the SLC22A5 gene, p.(Arg282Gln)—rs386134210, CM061983- in a young male infant. The detected variant was the only one of our cohort that was possible to classify as pathogenic according to the ACMG guidelines. Although the inheritance pattern is autosomal recessive, this variant has been classified as pathogenic, despite not being found in the homozygous or compound heterozygous form. Indeed, the presence of an additional P or LP variant in trans in the unanalyzed regions of this gene not covered by the custom panel performed in the current study should be considered. Therefore, an additional rare variant in the same gene is necessary to be considered causative of systemic primary carnitine deficiency disease. This variant characterized by a low allele frequency is more common in patients with Systemic primary carnitine deficiency (CDSP) than in the general population (PM2_Supporting; PS4_Supporting). In ClinVar database, it is reported several times as pathogenic significance. Functional in vitro studies [49] revealed the damaging effect on chinese hamster ovary (CHO) cells in comparison to controls (PS3_Strong). SLC22A5 gene encodes for the plasmalemmal carnitine transporter and the related disease encompasses a broad clinical spectrum including metabolic decompensation, cardiomyopathy, hypoglycemic hypoketotic encephalopathy or absence of symptoms [50, 51]. Progressive -both dilated and hypertrophic- cardiomyopathy are observed mainly in childhood, while arrhythmic events with shortened QT interval are described in adult people [52]. Roussel et al. [53] observed that the shortening of the QT interval at continuous electrocardiographic monitoring correlated negatively with plasma carnitine concentration causing ventricular fibrillation. These findings strongly suggest that long-chain fatty acid β-oxidation may influence the morphology and the electrical function of the heart leading to unexpected sudden death.
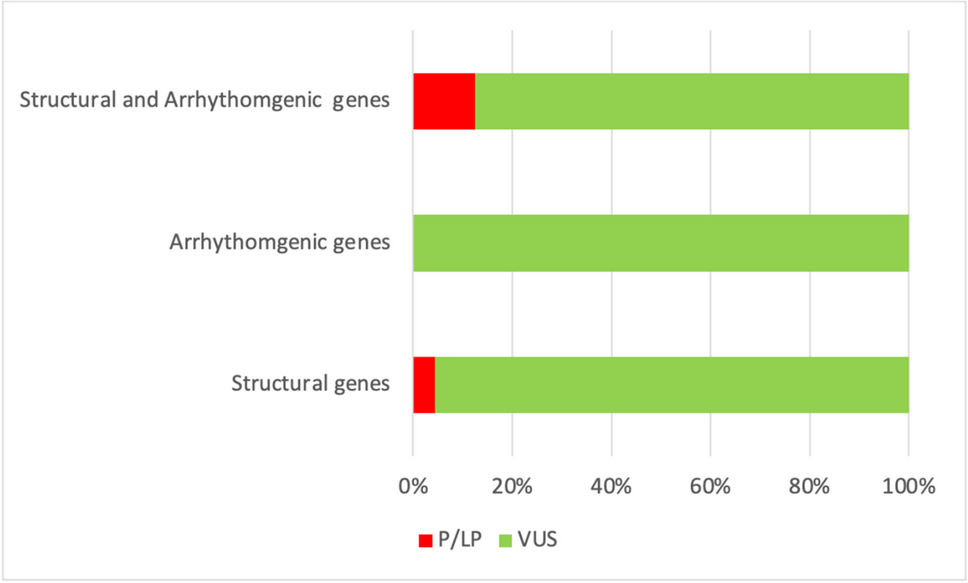
All above mentioned P/LP variants were found in structural or structural/arrhythmogenic genes. Despite the apparent greater involvement of structural genes compared to other gene groups, the difference in the distribution of variants was not statistically significant (chi square, p = 0,219) (Fig. 1).
The results of our analysis revealed that 5.3% of our cases exhibited at least one potentially causative variant, which could account for sudden and unexpected infant death. These findings are consistent with similar studies, such as those conducted by Tester et al. [9], who obtained comparable results by identifying pathogenic or likely pathogenic variants in 4.3% of 419 SIDS cases, even if with a minor allele frequency < 0.00005. However, in other studies, this percentage may reach up to 34% when filtered with a higher allele frequency, typically < 1% [54].
The evidence reported in our study support the utility of post-mortem genetic testing in cases of SIDS. However, the main challenge of the most advanced and comprehensive postmortem genetic analyses lies not in the technical identification of variants but in the interpretation of pathogenicity, assigning the variant a causal role in the infant's death. The identification of a variant as pathogenic has important implications for the relatives, so the clinical translation of laboratory results should be carried out carefully and a co-segregation analysis in the family members is highly recommended. The importance of segregation analysis among family members is well recognized in the scientific literature, as highlighted by European recommendations [55] for investigating SCD in adults and similarly emphasized by Kotta et al. [56] concerning sudden infant and early childhood death. In the current study, upon receiving the genetic study results from the Institute of Legal Medicine, family members were informed about the opportunity for clinical and genetic testing at a specialized unit for familial cardiopathies.


留言 (0)