Unlike traditional forensic medicine that often relies on singular observations during autopsies, research within clinical forensic medicine benefits from being able to employ experimental study designs akin to those used in clinical trials. For instance, the majority of research investigating the effectiveness of ALS compared to CWL, involve randomized study populations, controlled bruise inflictions, and examination strategies using multiple contact points with blinded assessments.
From an initial search encompassing 4055 records, ten articles were identified to meet the specified inclusion and exclusion criteria post screening. Data extracted from the selected studies indicate that employing a 415 nm ALS combined with a yellow bandpass/longpass filter outperforms CWL in both bruise detection and visualization. While research in this area is restricted to a single study, findings demonstrate that the 415 nm/yellow filter combination also performs better than CWL and other narrowband wavelengths when assessing bruises in individuals with darker skin tones. However, this is provided the location of a trauma is known. Only a single study compared the ability of ALS to discern bruising from non-bruising, with results indicating that caution is warranted if examining fluorescence [29].
Previous studies have raised concerns regarding the specificity of ALS in detecting bruising [29, 35, 36]. The chart review by Holbrook and Jackson [7] showcased an impressive capability of ALS to detect bruises, identifying bruising in 98% of reported cases of strangulation, wherein 93% displayed no apparent injuries under CWL examination. This highlighted the use of ALS as a compelling tool for bruise detection, with the findings presented in legal proceedings [29]. However, the absence of controls specifically addressing bruise validity limits the results [7], as ascertaining what the authors’ identified as bruising is perplexing, since neither hemoglobin nor bilirubin exhibit significant fluorescent properties, and skin may fluorescence from factors other than bruising [17, 37]. Further investigations by Lombardi et al. [29] revealed that a CWL had a significantly greater specificity compared to fluorescence under ALS. Authors concluded that the diagnostic reliability of fluorescence under ALS remains uncertain if bruising cannot be validated, and further investigation examining the specificity of absorption is necessary. Debatably, Lombardi et al. [29] presentation of results by pooling wavelengths into a single sensitivity and specificity measure may be deemed inaccurate, as data from individual wavelengths do indeed exhibit higher sensitivity and specificity than CWL at various time points during the course of the experiment. Nevertheless, to alleviate problems associated with the lack of specificity in routine casework, ALS examinations should always be conducted in conjunction with CWL. This approach facilitates the evaluation of additional factors including pain, swelling, and the patient’s history of physical trauma to validate bruising.
Moreover, common over-the-counter topical products have demonstrated to generate greater ALS absorption when applied on light or medium skin tones compared to those with dark skin [37]. One makeup product consistently absorbed wavelengths between 310 and 535 nm in 80.9% of observations, and sunscreen (SPF30) absorbed significant light in 7% of cases. However, the remaining twelve products tested absorbed light in less than 1% of observations [37]. In a follow up study evaluating the effectiveness of three different topical product removal methods (soap and water, isopropyl alcohol swab, makeup removal wipe), four out of 14 products continued to exhibit significant absorption after removal [38]. No differences were noted between removal methods, highlighting that further research exploring the specificity of ALS and topical products post-inflicted trauma is warranted, alongside studies questions relating to how previous wounds/scar-tissue, tattoos, moles (including Mongolian spots) and freckles affect specificity. Thus, live ALS examination is therefore advocated to ensure suspected bruises can be washed to mitigate any unknown risk of interference [17]. Relying solely on ALS and CWL photography for bruise examination may overlook such elements.
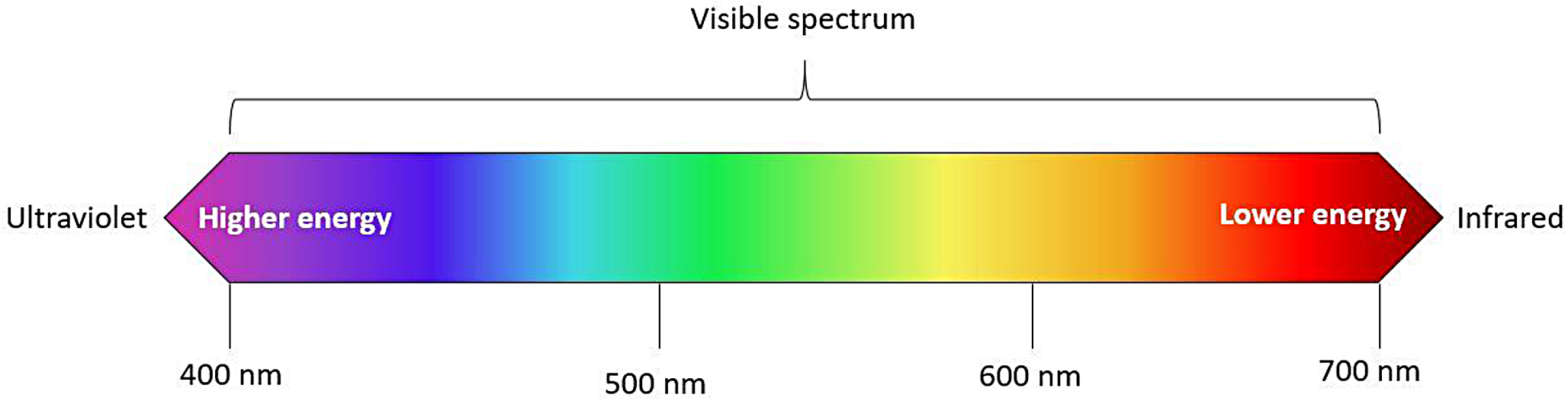
Research on the ability of ALS to detect and visualize bruising across varying skin pigmentations is sparse. Although Lombardi et al. [29] disclosed that subjects were recruited regardless of race, only a small fraction exhibited dark skin pigmentation. The majority of the selected studies examined white/light populations. Of the ten studies reviewed, only the study series by Scafide et al. [6, 8, 32, 33] has addressed equal representation across skin categories determined by spectrophotometry. Scafide et al. [6] found that the wavelengths 415 nm and 450 nm, when paired with yellow-cut filters, were consistently better than other wavelengths at bruise detection for all tested skin categories. UV was less effective than CWL in identifying bruising across darker skin tones, except in individuals with very light skin, which may be due to melanin’s peak absorption wavelength around 335 nm [39, 40]. On the other hand, hemoglobin’s absorption spectra typically exhibits a sharp peak at around 415 nm (dependent on oxygenation level) and most probably accounts for why the wavelength was most effective [19]. Although Scafide et al. [32] initially advocated the use of yellow or orange filters, subsequent analysis using the developed AVS [33], determined that yellow alone was more effective [6]. Although results are in contrast to findings by Sully et al. [41] who suggest that longer wavelengths combined with orange filters are superior in dark skin, the use of a goat model with topically applied melanin could have resulted in higher pigment concentrations than that of human skin and may account for differences observed. Additional studies are needed for further confirmation.
Furthermore, it should be noted that all ten studies examined bruising on extremities. The location of injury has demonstrated to have a significant impact on bruising manifestation and by extension, detection and visibility. For example, the presence of loose subcutaneous tissues increases the risk of blood extravasation, leading to more pronounced bruising around specific regions such as the eye compared to the hand [1]. Subpopulations such as children and the elderly are more susceptible to bruising than young and physically fit individuals [34]. Additionally, individuals with conditions like hypertension, diabetes, and coagulation disorders are also more prone to exhibit different bruising patterns. Certain steroids have been observed to affect the rate of bruising development [42], and common medications such as anticoagulants can influence both the formation and resolution of bruises, which can manifest immediately, or take longer to develop [1, 34]. Hence, results from the selected studies are constrained by the possibility that the data may not extend to injuries sustained on the torso, face/neck, and genital regions. In practice, medical history may not always be considered prior an ALS assessment, and further studies are warranted to address such injury mechanisms and locations.
While ALS research has primarily focused on assessing the technology’s capacity to detect and visualize bruising for enhanced documentation of blunt-force trauma for legal purposes, an ethical dilemma emerges regarding a potential for overinterpretation of injury mechanisms. Although this discussion falls beyond the scope of this review, it warrants attention for future research to contemplate how enhanced visualization of bruises could inadvertently mislead legal professionals lacking medical and technical expertise. For instance, an increased visualization could result in an overestimation of injury severity or mechanism of injury, leading to erroneous judgments and unjust outcomes in legal proceedings. Hence, forensic and legal experts must exercise caution and thoroughness when interpreting and communicating ALS bruising evidence, particularly if relying solely on photographs.
Limitations of study
This review faces several limitations stemming from predetermined constraints dictated by the nature of systematic reviews and the narrow research question. While studies examining both specificity and sensitivity were included, the strict criteria resulted in a restricted pool of eligible studies. Consequently, only ten studies were deemed suitable, with only a single addressing specificity. This selection bias should be considered when interpreting the review’s outcomes, as while ALS outperforms CWL in bruise detection and visualization, studies have only considered the technology where bruise location is known. In cases where a bruise cannot be validated either by CWL or other methods, ALS should be used with caution, as studies do not sufficiently address specificity.
It should also be mentioned that five out of the ten selected studies were authored by the same research team, four of which were derived from the same primary dataset. Such pseudoreplication of findings, albeit presented from varying perspectives, may be argued to pose a limitation to this review and the wider research domain.


留言 (0)