We conducted a prospective cohort study involving 38 infants and children with non-cancerous febrile neutropenia (61 hospital admissions with febrile episodes), who were receiving regular follow-up care in the pediatrics hematology and bone marrow transplantation (BMT) units of Cairo University Hospitals from December 2020 to January 2022.
Patients with febrile neutropenia, i.e., known cases of neutropenia resulting from bone marrow failure and presenting with fever (temperature equal to or above 38 °C), in the age range from 2 months to 18 years, both genders were included in the study.
Patients with neutropenia associated with hematological or non-hematological malignancies or transient neutropenia (e.g., due to transient viral infections) were excluded. The degree of neutropenia was classified as either severe, very severe, or non-severe (mild or moderate) based on ANC, as mentioned earlier.
The study participants underwent a thorough clinical assessment, including history and physical examination. Demographic data were collected, and the present illness was explored, focusing on symptoms, recent infections, and antimicrobial use. Physical examination covered vital signs, skin assessment, head and neck examination, central nervous system evaluation, cardiovascular examination, chest examination, gastrointestinal and renal evaluation. Anthropometric measurements were also recorded. This comprehensive approach provided a detailed overview of the participants’ medical history and physical health status.
The diagnostic tests included in the study were initially performed and subsequently repeated during the patients' admission period based on their clinical course progression.
The tests included the following:
1.
General laboratory tests: complete blood picture (CBC) with differential counts were done for hematological assessment, in addition to C-reactive protein (CRP) for sepsis screening. Also, liver function tests (alanine transaminase (ALT), aspartate transaminase (AST), total serum bilirubin level, and direct serum bilirubin level) and kidney function tests (urea and creatinine) were done.
2.
Microbiological tests for pathogen isolation: blood and urine specimens were sent for culture for each patient, other body site cultures such as wound swabs and hematoma aspirate according to patient presentation and clinical findings
For blood culture, two sets were sent for each patient; each set is composed of one aerobic and one anaerobic blood culture bottles for detection of bacterial and fungal infections (blood samples were withdrawn following strict aseptic precautions in pediatric), BacT/ALERT FA Plus and BacT/ALERT are standard anaerobic bottles. Bottles were labeled and sent immediately to the lab to be inoculated for incubation within the BacT/ALERT continuous monitoring blood culture system (BacT/ALERT 3D, bioMerieux Inc., Durham, NC, USA). The machine gives a positive signal in case of growth, prompt sub-culture, gram staining, and further processing was done.
Blood, Chocolate, and MaCconkey agar media (Oxoid, UK) were used for the culture of all specimens and Cled (Oxoid, UK) was used for urine. Incubation of culture plates, primary identification of growth by gram staining to gram-positive and gram-negative organisms, and further identification by biochemical reactions and interpretation were done following standard microbiological procedures according to the manual of clinical microbiology.
3.
Antimicrobial susceptibility testing: susceptibility testing for penicillins, combined penicillins, 3rd generation cephalosporins, 4th generation cephalosporins, aminoglycosides, vancomycin, macrolides, quinolones, linezolid, and lincosamides was done with gram-positive organisms, and for penicillins, combined penicillins, 3rd generation cephalosporins, 4th generation cephalosporins, carbapenems, aminoglycosides, quinolones, trimethoprim-sulphamethoxazole and colistin with gram-negative organisms. Antimicrobial discs used (Oxoid, UK) Antimicrobial susceptibility testing was done by Kirby disc diffusion methods for all antibiotics used except for vancomycin (vancomycin screen agar was used) and colistin, (colistin dilution agar was used). Interpretative criteria were done according to Clinical Laboratory Standard Institute performance standards for antimicrobial susceptibility testing (CLSI, 2023).
4.
Other microbiological testing: Galactomannan test was done for fungal infection detection. Respiratory viral screen by nasal swab for SARS-CoV2 (severe acute respiratory syndrome coronavirus 2) PCR testing was conducted during the pandemic period (December 2020 to January 2022) for 53 patients’ febrile episodes.
Regarding the management of the admitted cases, in uncomplicated febrile episodes, our unit protocol was initiated “empirical monotherapy with piperacillin-tazobactam, cefepime, or meropenem”. For complicated cases or those exhibiting hemodynamic instability, a combination of vancomycin with one of the previously mentioned agents is employed. Additional considerations include Metronidazole for gastrointestinal symptoms and, for persistent fever beyond 4–7 days despite broad-spectrum antibiotics, antifungal therapy. Should patients fail to respond clinically, or exhibit sustained high CRP levels, the protocol advocates transitioning to culture-based therapy guided by positive blood cultures or other positive cultures, such as urine or wound cultures.
Analysis methods
Data were analyzed using IBM SPSS advanced statistics (Statistical Package for Social Sciences), version 24 (SPSS Inc., Chicago, IL, USA). Numerical data were presented as medians and interquartile range (IQR), while categorical data were expressed as numbers and percentages. Comparison between multiple groups were compared using the Kruskal-Wallis test, and the Mann-Whitney U test was employed for pairwise group comparisons. The chi-square test was utilized to compare categorical variables.
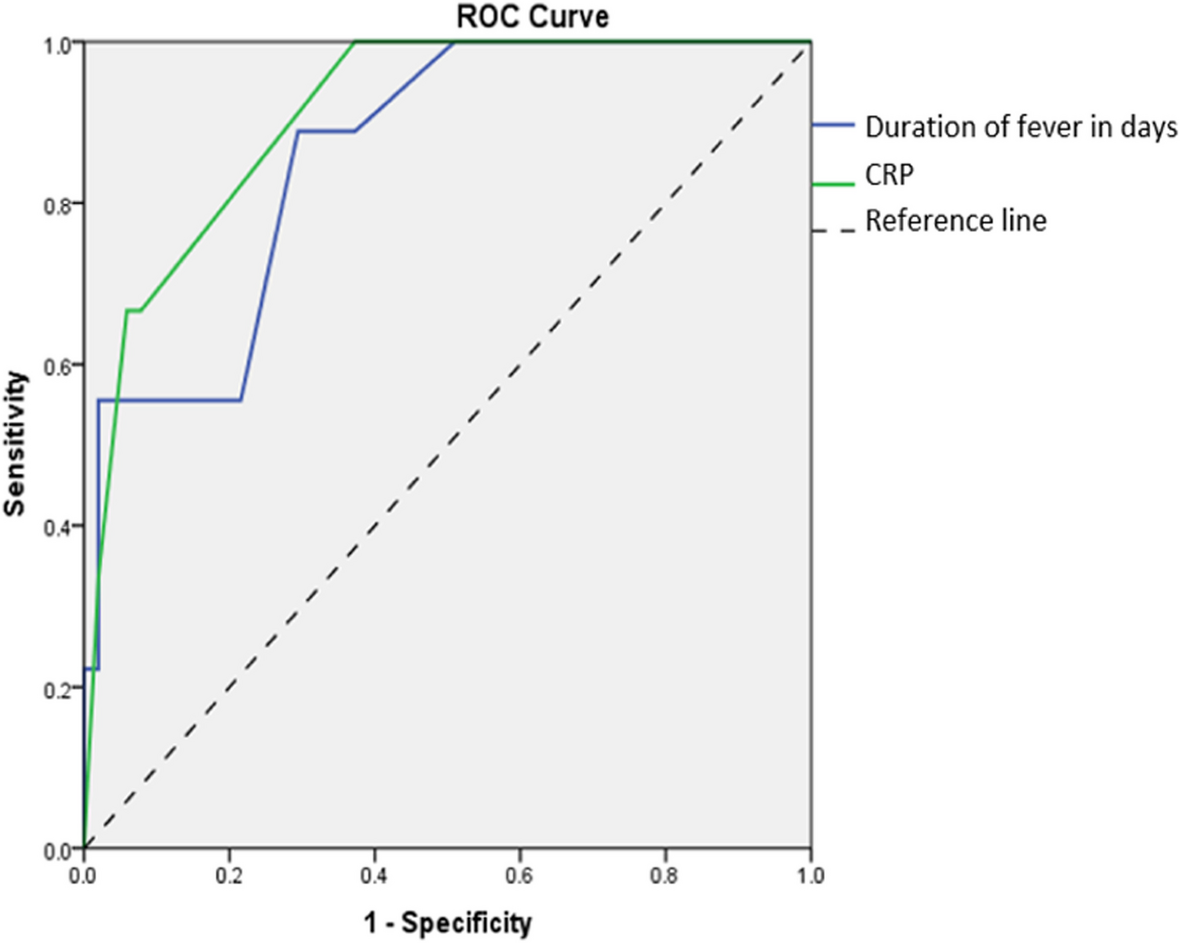
Additionally, a receiver operating characteristic (ROC) curve analysis was conducted to identify predictors of mortality during hospital admissions. In all analyses, statistical significance was defined as a p value of ≤ 0.05, and all tests were two-tailed.


留言 (0)