
記住我









Over the last decade, the role of nuclear imaging methods has become increasingly pivotal across a diverse range of clinical conditions, and notably so in the realm of oncology [1]. These imaging techniques have emerged as indispensable tools for precisely assessing the extent of disease, particularly in situations where conventional diagnostic methods may prove inadequate [1]. The realm of endocrine diseases presents a multifaceted clinical landscape, characterized by a wide spectrum of presentations and endocrine malignancies span from indolent to highly aggressive tumors, respectively [2]. This inherent complexity demands innovative and sophisticated approaches to diagnosis and management. The evolving landscape of medical imaging has witnessed remarkable progress, thanks in part to the introduction of novel medicinal radiopharmaceuticals and the continuous refinement of tomographic imaging technology [3]. In this context, Positron Emission Tomography/Computed Tomography (PET/CT) has garnered increasing attention and importance [3]. The integration of cutting-edge radiopharmaceuticals and the advancement of tomographic imaging techniques have substantially expanded the utility of PET/CT within the field of endocrine diseases [4]. The application of PET/CT now extends beyond conventional boundaries, offering healthcare professionals an enhanced ability to delve into the intricate nuances of endocrine disorders. This technology provides a comprehensive and multifaceted perspective on these conditions, enabling clinicians to make more informed decisions regarding diagnosis, treatment planning, response assessment and patient management [1]. As the field of nuclear imaging continues to evolve, PET/CT is poised to play an even more prominent role in addressing the complexities of endocrine diseases, ultimately leading to improved patient outcomes and a deeper understanding of these intricate medical conditions [5]. This article explores the latest advancements and research in the field of PET/CT, highlighting its growing role in endocrine disorders. Additionally, it analyzes the potential of personalized medicine in the field of endocrinology, where PET/CT is poised to make a significant impact (Table 1; Fig. 1).
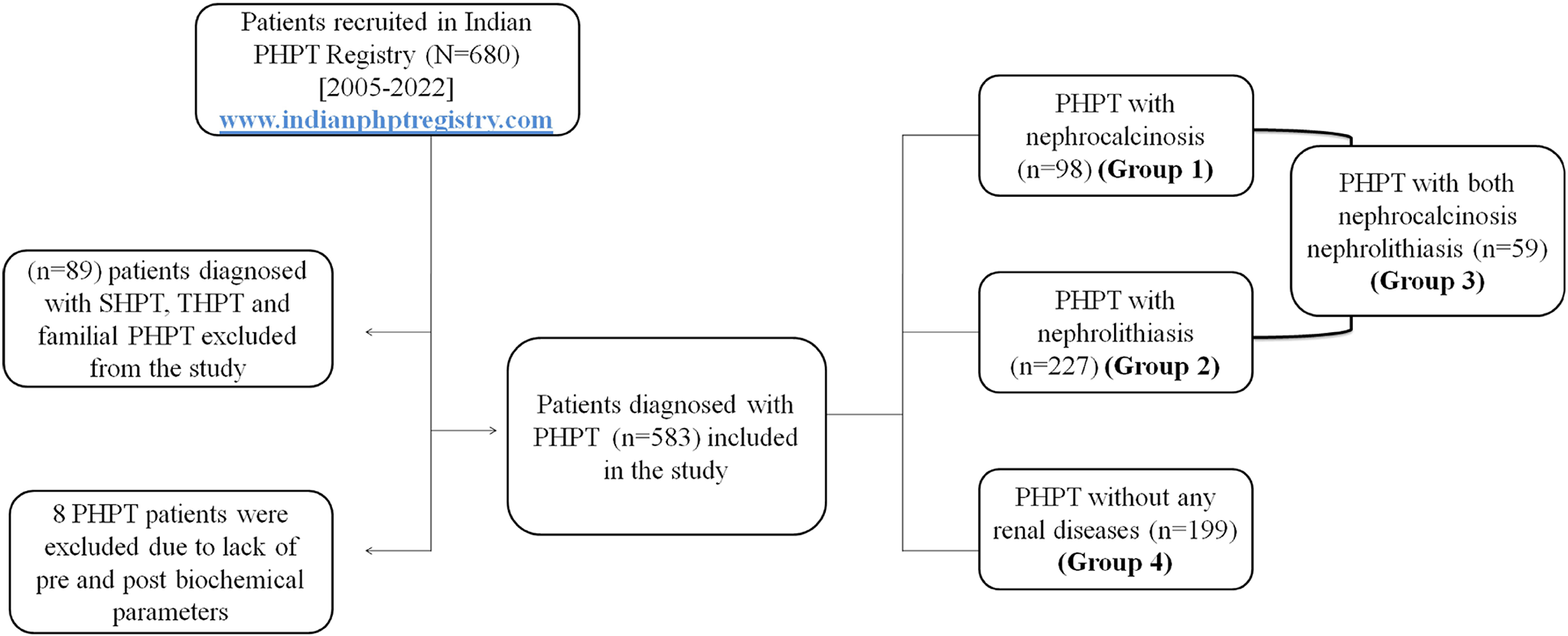
Table 1 PET tracers and clinical application in endocrinologyFig. 1
124I PET/CT of 63 yo woman with DTC after total thyroidectomy and RAI: (A) maximum Intensity Projection (MIP) multiple metastatic findings in the lung and upper mediastinum; axial images show metastatic lymph node in the upper mediastinum (B), multiple bilateral lung metastases (C–D) and a 3 cm solid mass in the right hilum of the lung (D); E 131-iodine scintigraphy findings after the second radioactive iodine (RAI) treatment: 131-iodine has accumulated in the metastatic tumor in the lungs and in the mediastinal lymph node
Positron-emitting radiopharmaceuticals and uptake mechanismPositron-emitting radionuclides find application in diagnostic imaging by emitting two monochromatic photons with an energy of 511 keV following a positron–electron annihilation event. Chemical forms containing positron-emitting radionuclides are generated by cyclotrons [6] (Table 2; Fig. 2).
Table 2 Proposed flowchart algorithm to use PET imaging to guide surgical managementFig. 2
[18F]FDOPA PET/CT preoperative staging in a 61 y.o. woman with hypercalcitonemia and mild elevation of serum CEA, showing focal uptake in thyroid nodule in the right lobe; no evidence of pathological lymph nodes. A MTC was diagnosed after total thyroidectomy
2-[18F]FDG2-Deoxy-2-[18F]fluoro-d-glucose (2-[18F]FDG) or [18F]FDG is a glucose analogue that enters cells through glucose transporters (GLUTs) and competes with glucose for uptake. When injected intravenously, it quickly spreads through body fluids and is taken up by various tissues through GLUTs, getting trapped inside cells [7]. Its distribution in tumor tissue is proportional to blood flow, and it’s transported into cells via facilitated diffusion by specific glucose transporters, especially GLUT-1. High GLUT-1 levels are associated with increased [18F]FDG uptake in human tumors and are also considered a marker of hypoxia, as tumor blood vessels often fail to meet local metabolic needs [7] (Fig. 3).
Fig. 3
Preoperative staging with [18F]F FDG PET/CT(A1) in a 32-year-old patient with a finding of a voluminous left adrenal mass: (A2) axial PET/CT images show an intense and inhomogeneous uptake in the adrenal mass and in some lumbar aortic lymph nodes; after left nephrectosurrenectomy and left lymphadenectomy, a diagnosis of high-grade ACC was made. B At follow-up PET scan, during mitotane therapy, was found a peritoneal carcinosis
[11C]choline and [18F]F-cholineCholine plays a crucial role in various biological processes, such as the synthesis of phospholipids in cell membranes, methyl metabolism, cholinergic neurotransmission, transmembrane signaling, and lipid-cholesterol transport and metabolism [8]. Choline-based PET tracers are substrates of phospholipid synthesis [4]. Tumor cells have a high demand for choline due to the rapid duplication of cell membranes, and they incorporate choline quickly to support this process [8]. Consequently, levels of choline and phosphorylcholine are elevated in many tumor cells, indicating increased choline uptake and phosphorylation. In slowly proliferating tumors, elevated phospholipid metabolite levels are associated with alterations in choline transport, incorporation, and utilization [9]. [11C]choline, biochemically identical to native choline, is commonly used for PET/CT imaging, particularly in patients with prostate cancer and other malignancies that do not exhibit GLUT system overexpression [9]. Physiological uptake of [11C]choline is observed in various glands (pituitary, salivary glands, pancreas), as well as in the liver, kidney, bowel, and stomach [8]. However, the short physical half-life of 11C (20 min) restricts its use to PET centers with on-site cyclotron facilities [10]. To address this limitation, 18F-labeled choline analogs, such as 18F-fluoromethylcholine, have been developed, mirroring the metabolic processing of native choline and serving as commercially available PET imaging agents [10] (Fig. 4).
Fig. 4
A Double tracer 99mTc-sestamibi and 99mTc pertechnetate in 71-year-old patient with primary HPT (PTH 226 pg/ml) and no evidence of enlarged parathyroid on ultrasonography and 4D CT; B SPECT/CT shows no findings likely to be an adenomatous parathyroid. C–D [18F]F-choline PET/CT MIP and axial images show the presence of small area of focal hyperfixation at the left upper parathyroid
124I e other iodine-analogsVisualization of NIS (sodium-iodide symporter) expression through in vivo molecular imaging has traditionally relied on diagnostic [123I or 131I] or post-therapeutic whole-body scans using [131I] [4]. An alternative long-lived PET radionuclide that is gaining increasing attention for clinical and long-term PET studies is iodine-124 (124I), which has biochemical behavior identical to other iodine isotopes, combining tracer specificity with high resolution of PET/CT [5].
The spatial resolution of images using this radionuclide is comparable to that achieved with more conventional PET tracers and its half-life of 4.2 days is suitable for imaging slow physiological processes, aided by the elimination of non-specific radioactivity, therefore appears to be the most promising iodine isotope for individual pretherapeutic dosimetry [5].
Finally, new radiopharmaceuticals are being developed for iodine pathway tracing, including [18F]tetrafluoroborate ([18F]TFB) and [18F]fluorosulfate ([18F]FSO3) [13]. From a technical perspective, the development of fluorinated tracers offers advantages such as easier labeling, improved image quality, and high tumor-background contrast in both animal and human studies [13]. Biologically, [18F]TFB and [18F]FSO3 are analogues of iodine, but they do not undergo the process of organizing iodine in thyroid cells [14]. Furthermore, they offer practical advantages as they use an easily synthesizable radiotracer fluorine-18, which is more accessible and economical than 124I [14].
[11C]methionine and [18F]FDOPAIn the past, the most widely used amino acid for PET tumor imaging was [11C]methionine [4]. Although the precise method of uptake by tumor cells remains somewhat unclear, it likely involves the transport of substrates across the tumor cell membrane [19]. [11C]methionine has been used primarily for the study of brain tumors, where the use of [18F]FDG can be problematic due to physiologically high uptake in normal gray matter of the brain [4]. The amino acid dihydroxyphenylalanine (DOPA) can be labeled with 11C to produce the tracer [11C]DOPA or with 18F to produce 18F-DOPA)[4]. As l-DOPA is the precursor of the neurotransmitters dopamine, norepinephrine and epinephrine, 6-[18F]FDOPA ([18F]FDOPA) enters the catecholamine metabolic pathway in both the brain and peripheral tissues [4]. In cases of heightened activity of l-DOPA decarboxylase [18F]FDOPA PET/CT is a valuable instrument [10]. [18F]FDOPA enters cells via amino acid transport systems (LAT1) for large neutral amino acids, which are present in almost all cells [10]. The enzyme aromatic amino acid decarboxylase (AADC) metabolizes 18F-DOPA into 6-18F-fluorodopamine, which in turn can be stored in secretory vesicles by the vesicular monoamine transporter (VMAT), thus effectively becoming trapped within the cell [10]. Clinical applications of PET/CT using [18F]FDOPA includes assessing the degeneration of presynaptic dopaminergic neurons, particularly in conditions like Parkinson’s disease [10]. It is also utilized for oncology, in particular imaging brain tumors and visualizing well-differentiated neuroendocrine tumors (NETs) such as medullary thyroid cancer, pheochromocytoma, paraganglioma, and congenital hyperinsulinemic hypoglycemia. Physiologically, [18F]FDOPA accumulates in the basal ganglia, liver, pancreas, adrenal glands, gallbladder, biliary tract, kidneys, ureters, and urinary bladder [10].
[68Ga]-DOTA-peptidesThe [68Ga]-DOTA-peptides ([68Ga]Ga-DOTANOC, [68Ga]Ga-DOTATOC, [68Ga]Ga-DOTATATE) exhibit high expression of somatostatin receptors (SSTR) [11]. Therefore, such PET probes allow the evaluation of the extent of disease and the suitability for peptide receptor radionuclide therapy (PRRT) in patients with differentiated neuroendocrine neoplasms (NETs), as well as the assessment of response, optimization of the treatment sequence, feasibility of PRRT-retreatment, and combination of PRRT with other therapeutic options [11]. In this setting, PET/CT has become an essential tool, since such a heterogeneous group of tumors arising from neuroendocrine cells can arise throughout the body, accurate localization and staging are essential for optimal management [12]. PET/CT has the advantage of detecting even small lesions and assessing their receptor expression in vivo [12].
PET/CT applications in clinical endocrinologyPET/CT in parathyroid disordersPrimary hyperparathyroidism (pHPT) is the third most common endocrine disease, in most cases due to inappropriate secretion of parathyroid hormone by one or more parathyroid adenomas [15]. Minimally invasive parathyroidectomy represents standard of care in pHPT as it can lead to clinical complications (hypercalcemia, kidney stones or osteoporosis) [16], even though asymptomatic at diagnosis in 80% [17]. Precise preoperative identification of parathyroid adenomas is crucial because minimally invasive surgery reduces surgical complications and expedites patients’ recovery therefore preoperative imaging for parathyroid adenomas is of great importance [18]. In secondary hyperparathyroidism (sHPT) surgery is not recommended, while patients with tertiary hyperparathyroidism (tHPT) often undergo total or subtotal parathyroidectomy, therefore the identification of adenomatous glands may be useful to assist surgical planning [19]. Furthermore, persistence or recurrence of HPT after parathyroidectomy occurs in approximately 5–10% of patients [20]. Normal parathyroid glands are rarely detected at cervical ultrasound (US) while enlarged hyperfunctioning ones (i.e. adenoma, hyperplasia) are detectable in a significant proportion of pHPT patients making US the first-line preoperative localization method [21]. However, US sensitivity varies considerably, from 55 to 88%, and depends on factors such as the experience of the examiner, the size of the adenoma, the presence of ectopic lesions, coexisting multinodular goiter, and the presence of enlarged cervical lymph nodes [22]. Second-line nuclear-medicine imaging is challenging because a radiopharmaceutical with specific uptake in hyperfunctioning adenomas is missing, therefore scintigraphy with [99mTc]Tc-sestamibi with Single Photon Emission Tomography/CT (SPECT/CT) is currently in routine use where available, with sensitivity values of 80% according to some authors [23]. In the latest guidelines for parathyroid imaging, the European Association of Nuclear Medicine (EANM) emphasized the prominent role of 99mTc-MIBI as the primary imaging tracer for pHPT, suggesting that the combination of SPECT/CT with cervical US can achieve a remarkable sensitivity of up to 95% to detect functional parathyroid glands [24].
It is important to note that [99mTc]Tc-sestamibi SPECT/CT may show false-positive results in case of benign thyroid nodules (especially oncocytic adenomas) and thyroid malignancies and false-negative results for small, cystic or necrotic parathyroid adenomas [25]. According to literature after negative or inconclusive conventional imaging, several PET radiopharmaceuticals may be useful second line agent in pHPT [25, 26]; [11C]methionine and choline-radiolabelled drugs are reliable with good specificity and sensitivity values. According to literature methionine PET/CT showed an overall high sensitivity and positive predictive value (PPV), underscoring its potential for facilitating minimally invasive parathyroidectomy [27]. Furthermore, [18F]F-fluorocholine PET/CT may offer an even greater level of diagnostic accuracy, improving the overall detection rate to 97.9% according to some Authors [8, 27, 28].
All in all, [18F]F-choline PET/CT is now considered the imaging method of choice in patients with tHPT due to its superior detection capability, also in cases of multiglandular disease and a low rate of localization failure of parathyroid adenoma [8]. Excellent sensitivity values of [11C]methionine PET/CT were also reported in the tertiary HPT setting, where multiple lesions were visualized in 57.9% of patients and ectopic lesions in 21.1% of patients [19]. According to Bijnens et al., [18F]F-choline PET/CT has proven to be a highly accurate method and obviates the need for extensive exploration in most cases where ultrasound and scintigraphy results do not align or both show negative results [21]. Nonetheless, its application in this context might face limitations because of cost and accessibility factors. These results highlight the promising role of nuclear imaging techniques, particularly [11C]choline and [11C]methionine PET/CT, in optimizing the precision and efficacy of parathyroid surgery, ultimately benefiting patients through reduced invasiveness and improved treatment outcomes. Further research and clinical evaluation are warranted to fully harness the capabilities of these advanced imaging modalities for enhanced patient care in the field of endocrinology. Table 2 shows a flowchart algorithm to use PET imaging to guide surgical management.
In the context of HPT, a brief mention must be made of brown tumors, abnormal bone repair processes resulting from HPT. The diagnosis of these lytic lesions in nuclear medicine is not uncommon, given their use in the management of both cancer and hyperparathyroidism [29, 30]. According to Jacquet-Francillon et al. [18F]F-fluorocholine PET/CT is preferable to [18F]FDG PET/CT, [18F]F-sodium-fluoride and in bone scintigraphy and it can simulate metastatic disease. The uptake of brown tumor appears reversible after parathyroidectomy, with a variable decrease depending on the type of disease [31].
Moreover, must be taken into account that other radiopharmaceuticals, such as [18F]FDG and [18F]FDOPA, can lead to false-positive findings in patients with HPT. For example, Terroir et al. report on a 43-year-old patient with MEN 2A suffering from hyperparathyroidism and medullary thyroid carcinoma (MTC). Two focal uptake areas within thyroid with [18F]F-DOPA were reported as multifocal MTC and two others in the central compartment of the neck as metastatic lymph nodes of MTC, however, post-operative pathological analysis revealed areas of multifocal intrathyroidal hyperplasia and two parathyroid glands [32]. Therefore, in case of coexistence of multiple endocrine diseases as in MEN 2A, the clinical finding must be carefully analyzed to correctly interpret [18F]FDOPA PET/CT.
Causing less than 1% of pHPT, parathyroid carcinoma (PC) is an extremely rare endocrine tumor (0.005% of all tumors) [33]. In 90% of cases, it is functional and secrete extremely high amounts of parathormone (PTH), but the clinical manifestations of PC are polymorphic, making diagnosis complex. The high recurrence rate and distant metastases are challenge with the most common distant metastases located in the lungs and liver. The usefulness of [18F]FDG PET/CT in assessing local recurrence and distant metastasis of PC is challenged. In contrast, [18F]F-choline PET/CT seems to be able to detect primary parathyroid carcinoma for preoperative localization and allow a one-stop-shop metastasis detection and whole body staging [34].
PET/CT in Thyroid DisordersRole of PET/CT in indeterminate thyroid nodulesThyroid nodules with indeterminate cytology, accounting for 25% of cases, include follicular lesions of undetermined significance or atypia of undetermined significance (Bethesda class III; malignancy risk ranging from 10 to 30%) and follicular neoplasms (Bethesda class IV; malignancy risk ranging from 25 to 40%) [35]. In clinical practice, it is common to repeat fine-needle aspiration biopsy (FNAB) and perform molecular tests in these cases [36]. Nevertheless, several authors are investigating whether certain radiopharmaceuticals, such as [99mTc]Tc-sestamibi and [18F]FDG, allow for the evaluation of the biological behavior and aggressiveness of “cold” thyroid nodules. If there is uptake of [99mTc]Tc-sestamibi and/or [18F]FDG, the calculated risk of malignancy is approximately 35%. Conversely, in cases of low or absent uptake of [99mTc]Tc-sestamibi and/or [18F]FDG, they are considered to have a very low risk of malignancy, demonstrating a high negative predictive value (NPV ~ 84 to 100%) [35,36,37]. High values of the maximum standardized uptake value (SUVmax), a semi-quantitative measure reflecting glucose metabolic activity, may be associated with an increased risk of malignancy. However, SUVmax is not a specific marker for malignancies, and therefore, no statistically satisfying specific threshold has been identified to distinguish malignant lesions. In addition, other PET-derived parameters, such as metabolic tumor volume (MTV) and total lesion glycolysis (TLG), have been examined, but the results lack consistent uniformity [35]. Some authors have shown a reduction in unnecessary surgeries thanks to [18F]FDG PET/CT [38]. De Koster et al. demonstrated that [18F]FDG PET/CT has high sensitivity values and negative predictive value (94.1% and 95.1% respectively) and that it is therefore a reliable tool to exclude malignant tumors and avoid unnecessary diagnostic interventions in thyroid nodules with indeterminate cytology [38].
Focal thyroid incidentalomasIncidentalomas are unexpected lesions discovered incidentally, usually not related to the original clinical indication for [18F]FDG PET/CT, and can be either focal or diffuse. In patients without known thyroid pathology, the prevalence of diffuse uptake is 0.1–4.5% and is usually related to benign processes such as chronic thyroiditis, Graves’ disease, while focal thyroid uptake ranges from 0.1 to 4.8% with an average malignancy rate of about 34% [39]. However, almost two thirds of focal [18F]FDG uptakes within the thyroid gland are related to benign diseases [39]. While focal thyroid uptake on [18F]FDG
留言 (0)