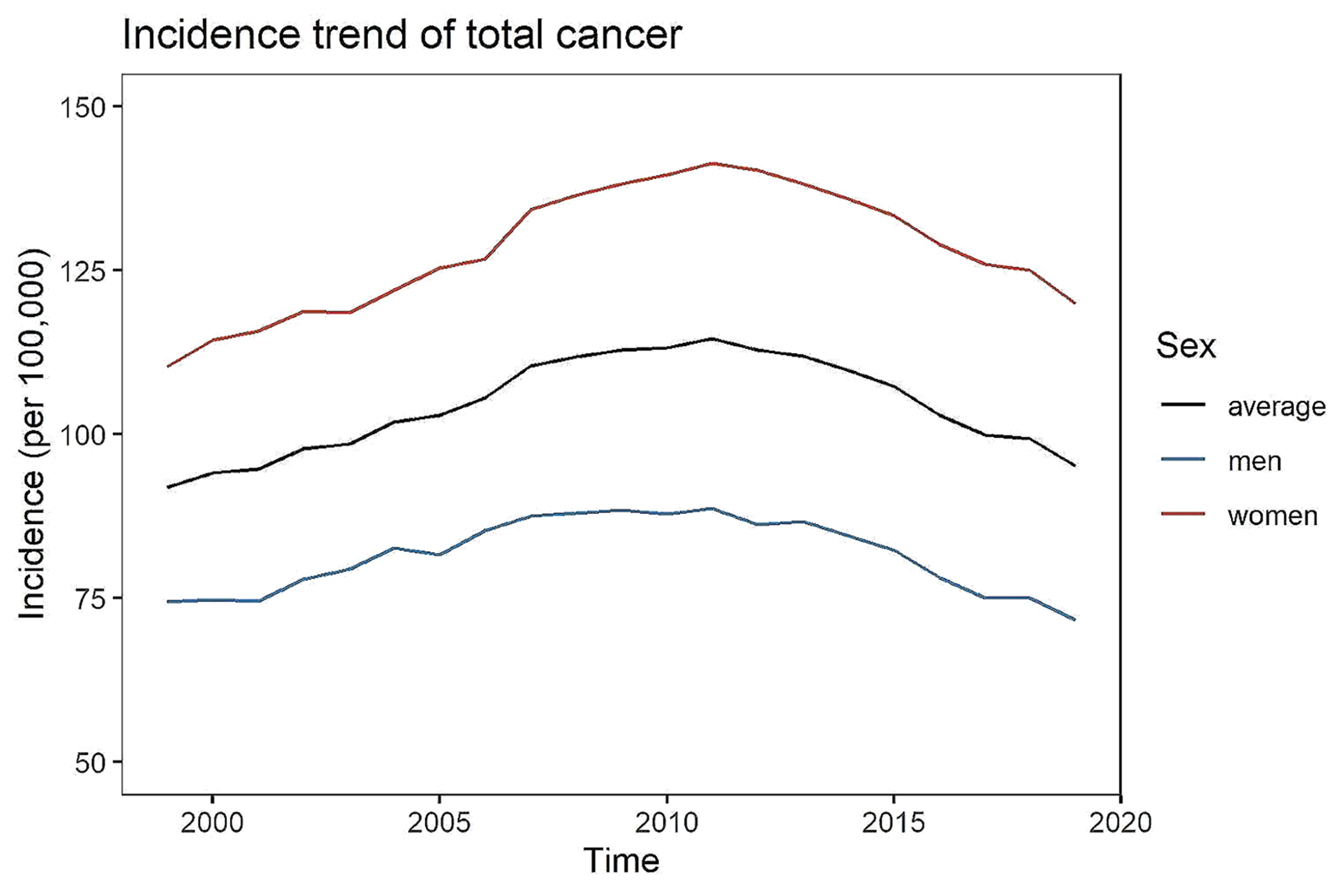
The aim of this study was to estimate temporal trends in the incidence and mortality of early-onset cancer in Germany between 1999 and 2019. Considering the total early-onset cancer incidence, cancer among younger ages is relatively rare compared to later-onset cancer. Our findings confirm that the incidence is higher as age advances. We observed stable or slightly increasing trends (0% and 1) in the incidence of all early-onset cancers combined (C00-C97) for men and women, respectively, and strict declines in the mortality for men and women (-3% and − 2%).
In Germany, there are no comparable studies on the epidemiology of early-onset cancer. However, the downward trend in the mortality is in line with reported findings on a global scale [1, 4]. Considering the trend in the overall incidence of early-onset cancer in Germany, this is partly conforming with global findings. Between 1990 and until about 2010, the incidence showed an upward trend, which is in line with trend analyses of the global early-onset cancer incidence identified by Lin et al. and Zhao et al. [1, 4]. Contrarily, in Germany since 2010, we noted a decrease in the incidence. This is unlike the findings of Lin et al. [4] and Zhao et al. [1], where the global incidence of early-onset cancer was found to have strictly increased between 1990 and 2019 (by 11% (Lin et al. [4]) and 79.1% (Zhao et al. [1])). With regard to the various, clinically heterogeneous types of early-onset cancer, our results are similar to those of Lin et al. [4] and Zhao et al. [1], seeing that among women, early-onset breast cancer had the highest incidence. Among men, Zhao et al. [1] report a maximum incidence for non-melanoma skin cancer. However, non-melanotic forms of skin cancer (light skin cancer) were not considered in our study due to a lack of data. Our analysis showed that in Germany between 1999 and 2019, malignant neoplasms of male genital organs had the highest incidence. Regarding mortality, early-onset cancer of the eye, brain and other parts of the central nervous system had the highest mortality among women in Germany, which is again in line with Zhao et al. [1] and Lin et al. [4] and their global estimates. For men, the highest mortality in Germany was found for early-onset cancer of digestive organs, while on a global scale, tracheal, bronchus and lung cancer had the highest mortality [1]. However, a recent German study confirmed a relatively high and rising incidence of early-onset colorectal cancer (ICD-10 C18-C20, i.e., part of our classification ICD-10 C15-C26 representing cancer of digestive organs) for the period 1999 to 2018 [2]. Overall, the observed differences between the global findings and our findings for the German population are logical, referring to substantial scientific evidence of considerable variation in the incidence and mortality of early-onset cancer among different areas, ages, countries, genders, and cancer types [1, 4].
As there remains debate about the optimal statistical method for analysing and predicting potential trends over time in cancer-registry data [15, 22], we applied three different statistical methods (negative binomial, Poisson and joinpoint regression). All three methods return comparable outcomes, i.e., negative binomial and Poisson regression return the annual percentage change while the joinpoint regression returns the AAPC. The rationale for applying the three methods is as follows. In epidemiology, Poisson regression is a common methodological choice for assessing trends e.g. in incidence or mortality. As discussed by Alsadhan et al. [22] the second most common statistical method for measuring trends in incidence in cancer registries was Poisson regression. Compared to Poisson regression, negative binomial distribution has one additional parameter and by that, accounts for overdispersion, i.e., it adjusts the variance independently from the mean. With regard to joinpoint regression, we report the AAPC which summarises the average Annual Percent Change (APC) over a period of multiple years in a single number and which is claimed advantageous over the APC [18,19,20]. First, it does not necessitate linearity of the trend. Second, the AAPC is able to characterize a much longer time series even when the data are sparse. Third, resulting AAPC are discussed as more stable. Fourth, the AAPC is claimed valid even if the joinpoint model indicates changes in trends during the respective time horizon as it is computed as a weighted average of the APCs. Fifth, as single summary measure it increases clarity and better comparability of the results [18,19,20]. However, modelling trends using piecewise linear segments on a log scale as done by joinpoint regression comes with some limitations (e.g. vs. Poisson or negative binomial regression), such as its inability to deal with missing data and zeros (e.g., in case there are no diseased in a particular cohort, which is not unlikely) [15], its application is much more time consuming [18] and unlike joinpoint regression, Poisson and negative binomial regression additionally return an estimated effect of age on trends in incidence and mortality.
Causes of the observed cancer burden
The causes for the observed burden of early-onset cancer have not yet been elucidated [1, 2]. Instead, there is growing evidence that the reasons and risk factors are multifactorial with differences between the specific cancer types, sex and age, demographics, society, economy, and lifestyle [1, 2, 4, 5]. For instance with regard to sex and on overall level, i.e. for all cancer types combined, we found an increase in the incidence among women and a stable incidence among men. The ZfKD argues that this difference is mainly due to sex-specific trends in respiratory and intrathoracic organs (C30-39), mostly lung cancer (C34), and other cancers promoted by cigarette smoking, which have been decreasing for men (by 3% in our study) [23]. Furthermore, changes in the environment (e.g., higher pollution rates) combined with the Western lifestyle and diet (e.g., high consumption of red meat, animal fats, refined carbohydrates, alcohol) and the resulting increases in obesity and physical inactivity are likely to have affected (and potentially increased) the incidence of early-onset cancer [1, 4, 23, 24]. Moreover, exposure to the mentioned risk factors already in early life or young adulthood might be another reason for the rising incidence of early-onset cancer. The exposure to such risk factors has likely caused the increasing incidence for both sexes (e.g., breast cancer (C50), thyroid and endocrine glands (C73-C75), Hodgkin Lymphoma (C81), Non-Hodgkin Lymphoma (C82-88), multiple independent sites (C96) for men and women; and increases in cancer in melanoma (C43), soft tissue (C45-49), male genitals (C60-63), myeloma (C90) among men), at least to a certain extent. Another reason for increasing incidence for some cancer types may be the promotion of cancer screening strategies, such as the worldwide extensive application and promotion of mammography screening between 2005 and 2015 [1, 4]. For instance, after the introduction of mammography screening in Germany in 2009, there is substantial evidence for an increase in the breast cancer (C50) incidence among the screened age-groups [25]. This may explain part of the increase in the incidence of early-onset breast cancer (C50) found in our analysis.
However, although there is an increasing uptake of screening and early detection activities, only few of the screening strategies for detectable cancers aim at individuals who are aged younger than 50 years [26]. For instance, only men aged 45 and over are eligible for prostate cancer screening, colonoscopy is available for women and men aged 55 years and over and mammography is offered for women aged between 50 and 70 years [26, 27]. Presumably, this explains a major part of the stable incidence rates of prostate cancer (C61) and colorectal cancer (C18) we observed in our analysis. Further, participation in cancer screening in Germany is voluntary [26, 27]. With regard to mammography, the attendance probability of the German population in 2014 was about 50%, i.e., only half of the eligible German population [25]. In addition, some examinations and tests (individual health services, in German: individuelle Gesundheitsleistungen, abbreviated to “IGeL”) are not part of the statutory early detection program and costs have to be paid for privately [27]. These include for instance ultrasound examination of the ovaries and prostate or the inspection of blood or other bodily fluids in the laboratory. It is not inconceivable that particularly young adults who do not represent major risk groups are less willing to pay for such screening possibilities.
Similarly as for the increasing incidence for some cancer types, the decline in cancer incidence (observed among women for female genital organs (C51-C58) and unspecified sites of cancer (C76-C89); among men for lip, oral cavity and pharynx cancer (C00-C14), respiratory organs (C30-C39), urinary tract (C64-C68) and unspecified sites (C76-C80)) might be caused by a multitude of impacting factors. The strength and prevalence of risk factors as well as advancements in cancer screening implemented before or during the study period, it is important to consider latency effects, i.e. the temporal delay of a potential reaction to changes, which could impact the observed incidence trends. For instance, tobacco has a long latency (about 10 years) for its effect on lung carcinoma, whereas diet and nutritional factors, treatment and medication as well as screening are said to have shorter latencies (about 5 years) [24]. It is thus important to consider the time it may take to impact (both, reduce or increase) cancer incidence rates subsequent to a change. Particularly with regard to smoking, it is well known that tobacco increases the risk of cancer in respiratory and intrathoracic organs, but also at many sites other than the lung, the most common being the oral cavity, pharynx, larynx, oesophagus, and urinary bladder [23, 24]. In Germany, smoking bans have been in effect in all federal states since July 1, 2008. Subsequent reductions in tobacco consumption and (active and passive) smoking are thus the most likely cause of the observed decline in lung cancer and other tobacco-related cancers (e.g., respiratory and intrathoracic organs (C30-39), urinary tract (C64-68), unspecified sites (C76-80)) in our analysis.
Comparing the development of early-onset to late-onset cancer showed that on overall level, i.e., all cancer types combined (C00-C96), there is a substantial difference in the absolute level of the incidence. The incidence of late-onset cancer is almost four times higher compared to the incidence of early-onset cancer. However, the temporal trend developed similarly between 1999 and 2019. This might indicate that changes in risk factors, screening, cancer management or similar might have had larger impact on cancer incidence (for both, early- and late-onset) than different underlying biological mechanisms of early- vs. late-onset cancer. However, this inference should be made with caution. More detailed future research is required to make this statement with certainty.
As for the incidence, a number of factors may be responsible for the decrease in cancer mortality. Firstly, screening and the consequent earlier detection of symptomatic disease may have led to subsequent reductions in mortality. For instance, the efficacy of early breast cancer detection through mammography and clinical breast examination has reduced breast cancer mortality by up to 25% between 2009 and 2016 [25]. Secondly, treatment and cancer management (e.g., improved surgical technique, standardization of preoperative and postoperative care, medication) today are better, more effective and more easily available in Germany than they were three decades ago.
Implications for cancer management
The incidence and mortality were largely variant with regard to the different cancer types, sex and age. As a consequence, high focus should be placed on local characteristics and prevailing risk factors when formulating cancer prevention and treatment strategies. Further, although it seems that the incidence of early-onset cancer in Germany has decreased over the last decade, it should be noted that this is only the case for some cancer types. Consequently, future emphasis should be placed on cancer prevention and cancer health education, on increasing public awareness of the multitude of potential risk factors, and on developing effective and targeted screening strategies for the various cancer types. However, the mechanisms of several cancer types are not yet fully known or the known causes cannot be influenced. Therefore, efforts should be placed on future research of prevention opportunities, to increase the estimated 40% of all cancer cases worldwide which could be avoided through preventive measures [23]. For instance, primary focus should be placed on early prevention practices through promoting balanced and healthy nutrition, regular exercising, maintaining a healthy body weight, timely childbirth, and breastfeeding. There is substantial scientific evidence that for instance, consuming about 5 servings of fruits and vegetables per day inhibits the risk of colorectal carcinoma. Other changes in diet that should be promoted particularly among the youth are less alcohol consumption, reduced consumption of smoked, red and cured meats which are all known and modifiable risk factors. Furthermore, the widespread use of antibiotics can lead to changes in gut flora and affect the gastrointestinal microbiome. As such, these drugs function as cancer risk factor. It may be valuable to consider a stricter prescription process of pain killers and antibiotics, and making such drugs less easily available (particularly for children and young adults). Another modifiable risk factor are chronic infections. In Germany, about 4% of all incident cases per year are attributable to infections [23]. Vaccinations could aid in the first place to avert chronic conditions and by that, any subsequent cancer risk. This has been shown for the hepatitis B vaccination, as well as for the HPV vaccination. It may therefore be of value to promote vaccinations among the youth and to create incentives for being vaccinated early and regularly (in case repeated vaccination is required to maintain protection). Further efforts should be placed on early detection of cancer and making screening available for children, teenagers and young adults, too. For instance, the introduction of mammography screening in Germany in 2009 led to a substantial increase in the breast cancer (C50) incidence. On the grounds of these findings, it seems recommendable to establish early and regular routine screening activities for women and men at younger ages (i.e., far below the ages of 50 years), too. In addition, it might be valuable to extend cancer databases and to more extensively collect information on screening methods and their application. For example, tumour registries could be complemented by adding genetic and preventive information as suggested by Schmutzler et al. [28]. In doing so, the effectiveness of preventive measures based on validated risk factors and screening activities could be better evaluated in general as well as potentially, such information may provide evidence that allows for a transition from age- to risk-adjusted screening. Associations of smoking and tobacco consumptions with higher cancer risk have also been shown in numerous observational studies and have thus been identified as leading risk factors for cancer in respiratory and intrathoracic organs, but also at many sites other than the lung, such as the oral cavity, pharynx, larynx, oesophagus, and urinary bladder [23, 24]. Good efforts in reducing the tobacco consumption such as though the smoking ban since 2008 should be maintained, if not even extended. The passing of the cannabis act (Cannabisgesetz, CanG) in Germany in April 2024 legalises private cultivation of cannabis by adults for their own consumption and allows smoking joints legally. It is well known that cannabis may relieve many of the symptoms that can occur among cancer patients, including sleep problems, nausea, loss of appetite, weakness and pain [29, 30]. However, studies found an association of cannabis and lung cancer risk as well as a weakening of the body’s immune system, which in turn increases the susceptibility to infectious diseases and risk of cancer [29,30,31]. It may be wise to identify major consumer profiles (i.e., potential risk groups), to closely monitor the future cannabis consumption and to observe its consequences [31].
With regards to trends in mortality in Germany, the generally low and decreasing rates may be due to sufficient local medical resources, as well as effective prevention and control practices. Further, the observed reduction of cancer mortality may imply that earlier efforts in medical development and treatment activities have achieved good results in cancer management. Furthermore, it must be noted that despite decreasing incidence, a disease’s prevalence may increase, for instance, due to ameliorated medical care, improvements in disease treatment and/or a reduction in disease-related mortality. Our results should therefore not be mistaken as an indication of decreasing total cancer burden among young adults and the associated demand on healthcare resources. Consequently, it is key to maintain these efforts and to further invest in averting the burden of early-onset cancer in terms of cancer being the main disease hindering life expectancy.
Strength and weaknesses
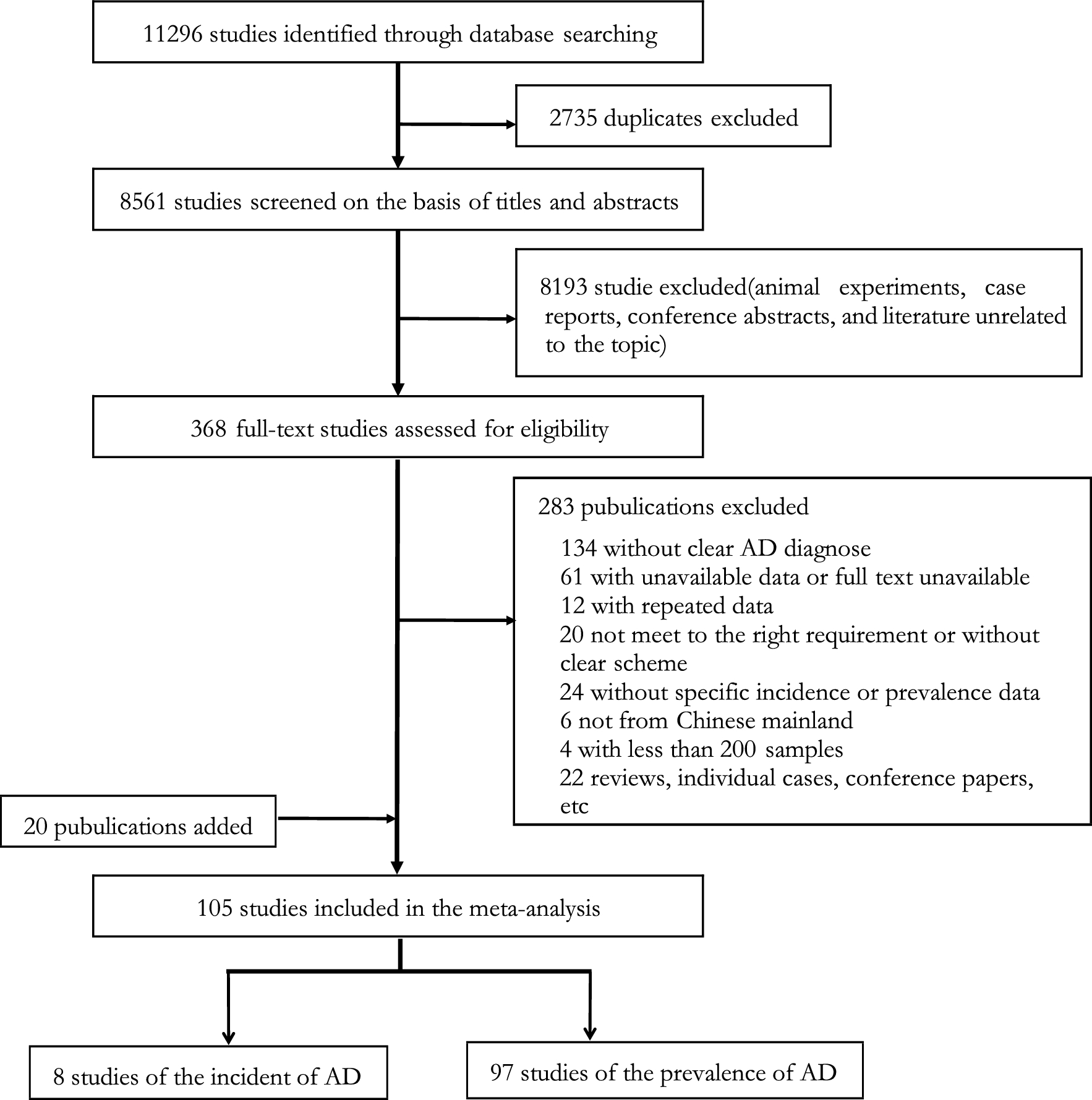
A main strength of our study is that it is based on nationwide registry data from the German population [9]. By contrast, one of the major limitations of previous is that the accuracy of GBD data was compromised by the quality, availability and representativeness of cancer registry data for the different countries. Hence, using data obtained from the Centre for Cancer Registry Data (Zentrum für Krebsregisterdaten, ZfKD) our study overcomes this major limitation of previous global cancer studies. The described data enabled us to draw a relatively comprehensive and unbiased picture of temporal trends in the incidence and mortality of diagnosed early-onset cancer in Germany for a long observation period of two decades. Another advantage is that our analysis differentiates by sex and age, as well as by cancer type. Knowing that cancer combines several heterogeneous subtypes in terms of different aetiologies, physiologies, risk factors, and treatments, our findings quantify and clarify the burden of the specific cancer types for each sex. Lastly, we applied three different statistical models to estimate the potential trends. The results from all methods are consistent and validate the respective findings.
However, the present study is subject to some limitations that are mostly related to our input data. Firstly, with the passing of the Federal Cancer Registry Act (BKRG) in Germany in 1995, all German states are obligated to establish epidemiological cancer registries and pass their data to a national cancer registry. The law has greatly advanced cancer registration such that nowadays, the cancer registry data of the ZfKD has a sufficiently high coverage of over 90%. However, it does not (yet) achieve 100% completeness (see Table S6) and thus leaves room for some uncertainties in the representativeness of our estimates [9, 13]. Further, due to potential differences in the quality of the cancer registry data in the different federal states, under-recording or underdiagnosis may occur which may result in underestimation [32]. Secondly, the data does not allow for precise reflection on cancer survivors, i.e., people who are considered cured when having lived an average of five years after successful cancer therapy without recurrence [33]. We are thus unable to make any statements concerning the number of unrecorded cases, i.e., undiagnosed or not yet detected cancer. Consequently, we are only making statements about the rates and trends of diagnosed cancer. The total incidence of diagnosed and undiagnosed early-onset cancer is likely higher than our estimate since people with undiagnosed cancer are not considered in our estimation. However, this is only relevant and may impact the estimated temporal trend if the proportion of diagnosed compared to undiagnosed cancer cases has changed between 1999 and 2019. Thirdly, our input data was aggregated on population level and was differentiated only with regard to age and sex. Therefore, due to lacking information, we stratified our analysis accounting for sex and age only. However, other risk factors or covariates may be worth assessing in this context. Fourth, we aligned with the German cancer registry and the ICD classification with regard to the grouping of the different cancer types [5]. Knowing that cancer is a group of various subtypes which differ greatly by type and among different patients, it may be of interest to further split the groups and consider each type (C00 to C97) and its subtypes separately. For example, esophageal adenocarcinoma is different from esophageal squamous carcinoma as well as microsatellite instability-high colorectal cancer is different from non-MSI colorectal cancer. It may be possible that the grouping of different cancer types may mask significant increasing or decreasing trends in each cancer entity. Consequently, future studies that investigate the incidence and mortality of each early-onset cancer are warranted. This may be helpful to counteract the individual types of cancer more effectively and in a more tailored manner.

留言 (0)