Study design and participants
The MIND-ADmini trial was a 6-month proof-of-concept multicentre, randomized controlled parallel-group trial (three arms). A detailed trial protocol has been published previously [15]. Participants were recruited from memory clinics in Stockholm, Sweden, and Toulouse, France, via advertisement in Frankfurt Germany, and from the university hospital neurology clinic and previous research cohorts in Kuopio, Finland. Pre-screening was performed for some of the inclusion criteria where information was available. Inclusion criteria were: age 60–85 years; Mini-Mental State Examination (MMSE) ≥ 24 points; availability of a study partner; prodromal AD according to International Working Group-1 (IWG-1) criteria including episodic memory impairment and underlying AD pathology [2, 16]; and an index indicating potential for lifestyle improvement. We defined episodic memory impairment as -1 SD on at least 2 out of 8 tests, at least 1 being a memory test: Free and Cued Selective Reminding Test (FCSRT) delayed free recall ≤ 8, FCSRT free recall-learning ≤ 22, Wechsler Memory Scale-revised (WMS-R) story delayed recall ≤ 75%, WMS-R delayed recall figures ≤ 75%, Trail Making Test (TMT) A ≥ 60 s, TMT-B ≥ 60 s, symbol digit substitution test ≥ 35 (120 s), category fluency ≤ 16 (60 s). AD pathology was defined as having ≥ 1 abnormal cerebrospinal fluid (CSF, CSF β-amyloid (1–42/1–40) × 10 ratio < 1 and/or total-tau and/or phospho-tau and/or β-amyloid 42 based on local cut-offs) or neuroimaging biomarker (Scheltens medial temporal lobe atrophy score of at least 1and/or abnormal FDG-PET and/or PiB-PET compatible with AD type changes) [15]. A score of 2 or above was additionally required on a lifestyle index based on physical inactivity, unhealthy dietary habits, hypertension, diabetes, sleep disturbances, depressive symptoms or psychological stress symptoms [15].
Exclusion criteria were: dementia diagnosis; conditions affecting safe intervention engagement (e.g., exercise); concomitant severe diseases (e.g., recent history of myocardial infarction or cancer); major depressive disorder; MRI/CT scan indicating stroke, intracranial bleeding, mass lesion or normal pressure hydrocephalus; intake of vitamin B6, B12, folic acid, vitamin C and/or E supplements > 200% recommended daily intake unless prescribed by a physician; use of omega-3 preparations (> 500 mg EPA + DHA per day); alcohol or drug abuse; severe loss of vision or communicative ability; conditions preventing cooperation as judged by the study physician; and concomitant participation in any intervention trial.
Randomization and masking
Participants were randomized to lifestyle intervention, lifestyle intervention + medical food, or control group receiving regular health advice in 1:1:1 ratio in blocks of six (computer generated allocation, two individuals randomly allocated to each group) at each of the four sites after screening by the study nurse. Outcome evaluators were blinded to the randomization group and were not involved in intervention activities. Similar to the FINGER trial, group allocation was not actively disclosed to participants, and participants were instructed not to discuss the intervention with outcome evaluators.
Intervention
The control group received regular health advice. All participants met the study nurse at screening, baseline, and 6 months after randomisation for health measurements (e.g., blood pressure, weight and BMI, and hip and waist circumference). All participants met the study physician at screening and 6-month visits for detailed medical history and physical examination. At baseline, the study nurse gave all participants (control and intervention groups) oral and written information and advice on healthy diet and physical, cognitive, and social activities that are beneficial for management of vascular risk factors and disability prevention. In the case of clinically relevant abnormal blood tests (samples collected at baseline and 6-months), participants were provided with information and advice to contact primary health care or a referral to primary health care. All participants had a chance to contact the study nurse by telephone or e-mail when needed.
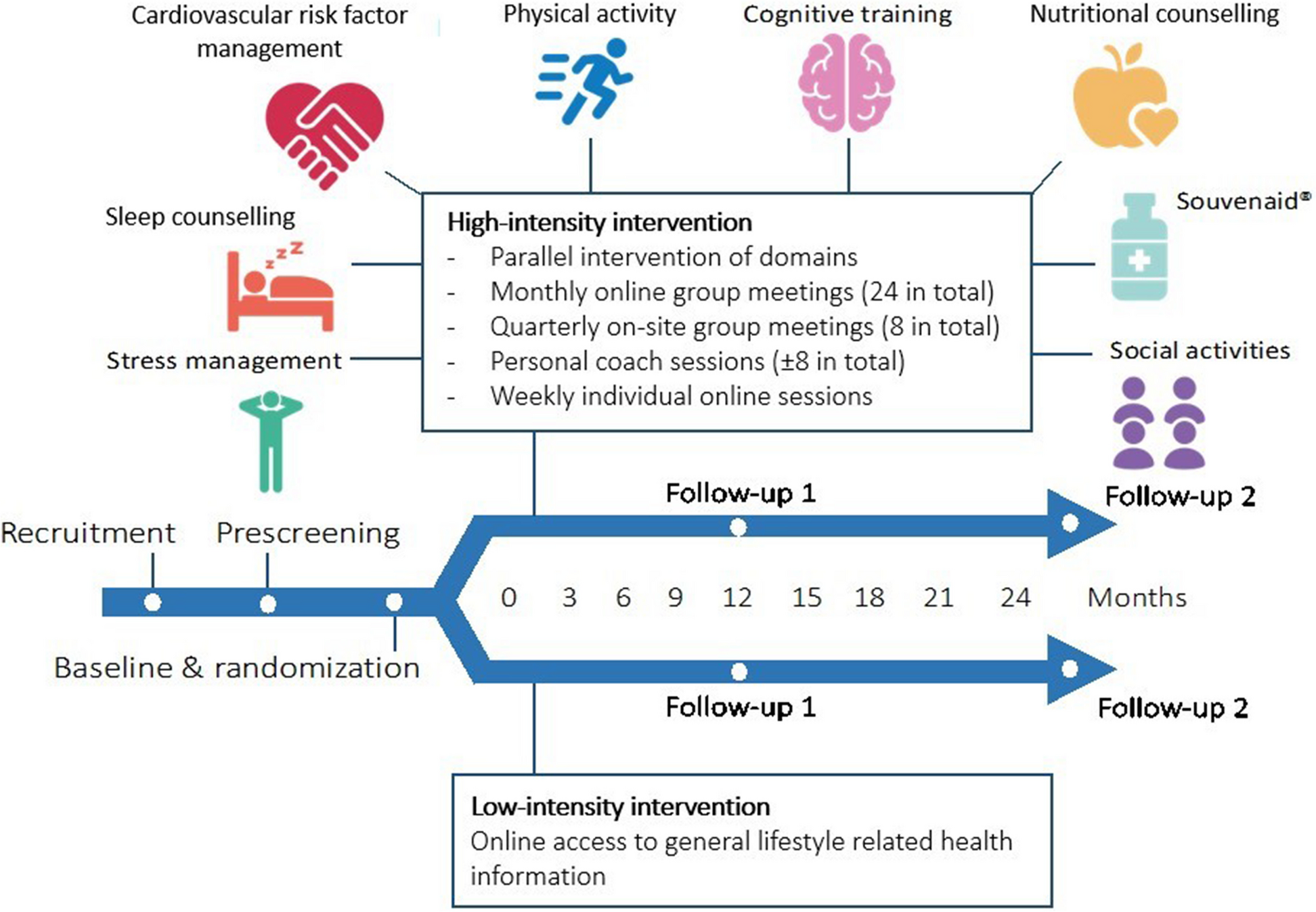
The multimodal lifestyle intervention group received a FINGER-based intervention program adapted for individuals with prodromal AD [15]. Intervention duration was 6 months. Stepwise introduction of intervention domains was used to promote adherence. Diet and physical activity started during the first month, cognitive training started during the second month following randomization. Given that intervention domains had both individual and group sessions, there could be a delay of up to 1–2 months before all domains were introduced. Intervention sessions and schedule were aligned among study centers to ensure similar intervention content and intensity for all participants, while leaving room for some local adaptations and flexibility [15]. Interventions were delivered in university facilities (Germany), and university hospital and private commercial gym facilities (Sweden, Finland, and France).
The FINGER-based lifestyle intervention combined five domains. Nutritional guidance, following the Nordic Nutrition Recommendations (NNR) 2012 or adapted to the country’s nutritional recommendations (France and Germany) [17], was provided by a registered dietitian/nutritionist through 3 individual counselling sessions and 3–4 group sessions. The physical exercise training program, supervised by a physiotherapist or personal trainer, was tailored to each participant’s fitness level and included cardiovascular endurance and progressive strength training [15, 18,19,20], Training sessions were conducted twice/week (60 min/session) with groups of 4–5 participants. Cognitive training included group and individual sessions. The 2–3 group sessions (60–75 min/session), led by psychologists or occupational therapists, included general information about neurocognitive disorders, coping and reasoning strategies, introducing the cognitive training program and instructing its use. Individual training sessions consisted of computer-based training at home or study site (twice/week, 15–30 min/session). The cognitive training program was a web-based, in-house developed computer program including several tasks adapted from protocols previously used in the FINGER trial [11, 15]. Social activities were stimulated through group sessions within the intervention domains (exercise, nutrition, and cognitive training), designed to facilitate open discussions and interactions among participants. Monitoring and management of vascular/metabolic risk factors, following national evidence-based guidelines, comprised one additional study nurse visit at 3 months, for blood pressure, weight and BMI, hip and waist circumference measurements, and further recommendations for lifestyle management, including smoking cessation. If medication initiation or adjustments were needed, the study physician either wrote a prescription or referred the participant to regular healthcare, as per local procedures.
The multimodal lifestyle + medical food intervention group received all lifestyle intervention domains mentioned above, plus the study product Fortasyn Connect (Souvenaid™), a 125 ml once-a-day milk-based drink including a complex nutrient combination (long-chain omega-3 fatty acids docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA), uridine monophosphate, choline, vitamins B12, B6, C, E, and folic acid, phospholipids, and selenium) designed to enhance efficacy over what can be achieved by individual nutrients. Danone Nutricia Research provided this study product for the MIND-ADmini trial.
Outcome measures
The primary outcome was feasibility of the multimodal intervention measured by recruitment rate, retention rate, and overall intervention adherence (in the 2 intervention arms). Recruitment rate was calculated by dividing the number of randomised participants by the number of potentially eligible participants who were invited to participate during a 6-month recruitment phase. Due to study sites having different start dates, recruitment rate was calculated considering the initial 6-month period at each site. A recruitment rate of ≥ 50% was pre-specified as successful [15]. Retention rate was calculated as the proportions of participants who completed the 6-month trial period. A successful retention rate was pre-specified as ≤ 35% of participants dropping out. Overall intervention adherence was calculated in the 2 intervention arms (multimodal lifestyle ± medical food) as a composite measure of participation in different intervention domains. The number of attended sessions was divided by the total number of sessions offered to the participants. Successful adherence to the lifestyle intervention was pre-specified as attending ≥ 40% of sessions/domain in at least 2/4 domains (exercise, nutrition, cognitive training and monitoring and management of vascular/metabolic risk factors); for the lifestyle + medical food arm, consuming ≥ 60% of the medical food study product was additionally required.
The secondary outcomes included adherence to specific intervention domains (in the 2 intervention groups), and adherence to healthy lifestyle changes (all participants). Adherence to specific intervention domains was computed as follows: Nutrition adherence was defined as attending at least 2 out of 3 of the group sessions, and 2 out of 3 of the face-to-face dietary counselling sessions. Exercise adherence was defined as attendance in at least 40% of the twice per week offered group-based gym sessions. Cognitive training adherence was determined by attendance in at least 2 out of the 3 group sessions, and automatic recordings of computer program use, i.e., number of completed training blocks divided by 48 (maximum offered number). Adherence to monitoring and management of vascular/metabolic risk factors was defined as attending 3- and 6-month meetings with the study nurse for cardiovascular health measurements. Medical food adherence was defined as consuming ≥ 60% of the medical food product based on diary information, i.e., bottles consumed divided by bottles delivered for each participant.
Adherence to Specific healthy lifestyle changes was calculated in all trial participants based on four domains: healthy dietary intake, physical activity, cognitive and social activities (considered as a single domain), and cardiovascular risk burden, measured at baseline and month 6. Healthy dietary intake was based on a modified Mediterranean Diet Adherence Screener (MEDAS) score calculated from the food frequency questionnaire, with a higher score indicating a healthier dietary intake [21]. Physical activity was measured actigraph-measured percentage of daily time spent on moderate to vigorous physical activity (ActiGraph GT3X, Pensacola, FL, USA); for 28 participants with missing actigraph data, the Swedish National Board of Health and Welfare self-reported physical activity questionnaire was used instead. Cognitive and social activities were quantified as self-reported engagement in different types of cognitive (i.e. studying, writing, crossword puzzles, hand crafts, course participation) and social activities (i.e. volunteering, engagement in a club/association, taking care of children, playing card and board games) [12]. Engagement in each activity was rated using a 7-point Likert scale of frequencies ranging from a daily to never, with higher score indicating more engagement. Overall cardiovascular risk burden was measured using the FINRISK score including age, sex, serum total cholesterol, systolic blood pressure, HDL-C, smoking status, and diabetes, with a higher score indicating higher cardiovascular risk [22]. Each participant’s overall cardiovascular risk score was divided by the overall cardiovascular risk score calculated for a sex and age-matched person without any cardiovascular risk factors, as previously defined [22]. Overall adherence to healthy lifestyle changes was calculated as a composite healthy lifestyle score, based on the specific healthy lifestyle changes, in all trial participants at baseline and month 6, by adapting a method previously used in the FINGER trial [23]. A score from 0 to 2 (with higher score indicating healthier lifestyle) was assigned to each tertile of the healthy dietary intake score, physical activity level, cognitive and social activities (lowest tertile = 0, middle = 1, highest = 2), and cardiovascular risk burden (lowest tertile = 2, middle = 1, highest = 0). The composite healthy lifestyle score was calculated as the sum of tertile scores in all four domains (ranges from 0 to 8).
Exploratory assessments
The Clinical Dementia Rating Scale (CDR) was used to evaluate cognitive-functional level at baseline and 6 months [24, 25]. The CDR-Sum of Boxes (SOB) score was calculated by summing the scores from each domain. An increased score on the CDR-SOB or global CDR score indicates more severe cognitive impairment. The range of the CRD score is 0–3 points, and the range of the CDR-SOB score is 0–18 points.
Statistical analysis
Because primary outcome measures focused on feasibility, formal sample size calculations were not performed. Analyses included all randomized participants, except for adherence to intervention measures which were limited to all participants randomized to the 2 intervention arms. Baseline characteristics were compared between trial arms using chi-square test (categorical variables) or one-way analysis of variance/Kruskal–Wallis test (continuous variables). Recruitment, retention and intervention adherence rates are reported using descriptive statistics. Differences from baseline to month 6 between trial arms regarding adherence to healthy lifestyle changes (overall and per domain) were investigated using linear mixed-effects models. This analysis adjusted for the cluster effect by capturing the correlation among participants within each site and accounting for individual variations within clusters and groups. We report estimates and 95% confidence intervals (CIs) for two-way interactions between randomization arms (control, lifestyle, and lifestyle + medical food) and time (baseline vs. month 6) in the linear mixed-effect models.
To evaluate differences between intervention arms (lifestyle or lifestyle + medical food) and the control arm in changes in the CDR-SOB and global CDR scores, we applied the generalized estimating equations with an ordinal logit model, with a robust variance estimator (cluster by each participant). We considered the CDR-SOB and global CDR scores as “ordinal” outcome measures because their mutually exclusive categories can be ordered by severity of cognitive-functional symptoms [26]. We estimated odds ratio (ORs) and 95% CI of two-way interactions between randomization arms (control, lifestyle, and lifestyle + medical food) and time (baseline v.s. 6 month) in the models.
All statistical analyses were performed in STATA 17.0 software by an independent statistician who was blinded to randomization.






留言 (0)