
記住我

This was a prospective cohort study, including all female patients presenting to the Paediatric Surgery Department, Cairo University Egypt, with persistent urogenital sinus secondary to CAH, in the period between May 2021 and February 2023.
All patients with persistent urogenital sinus had a contrast genitogram performed using Omnipaque® under fluoroscopy guidance, the same technique used in our centre in a previous study [14]. We used the measurements that were described and illustrated in other studies [14,15,16]. Patients were generally anesthetised either in the same setting of surgery or preoperatively in a different setting. A radio-opaque marker of known dimensions was placed at the perineum about 2–2.5 cm anterior to the limit of the anal verge. The positioning of the patient was done in an exact lateral position while putting both femurs precisely aligned together and pulling both thighs towards the patient’s abdomen. A 6F catheter was inserted into the external opening for just 1 cm.
Contrast material was injected under fluoroscopic guidance with moderate pressure until the confluence was delineated. If difficulty appeared in introducing contrast to the vagina, the catheter was manipulated by pushing, pulling, and rotation with an injection under a higher pressure by closing the external opening with the thumb and index finger to avoid leakage. The depth of confluence from the perineal marker was measured in ratio to the perineal marker dimensions, whatever the scale of the genitographic picture was, and measurements were taken in millimetres. Other measurements of the urethra proximal to the confluence, the vaginal dimensions, and the depth of the bladder neck were taken (Fig. 1).
Fig. 1
Genitography measurements. UB, urinary bladder; V, vagina; PU, urethral proximal to the confluence; solid line, confluence depth; dotted line, bladder neck depth
All cases were further investigated using rigid 9.5F cystoscopy with a thirty-degree lens. The scope was introduced along the UGS and advanced into the bladder. Most of the times, it finds its way easily to the bladder more than the vagina due to the narrow vaginal orifice and posterior location which make it better searched for in a retrograde pattern with high saline flow.
In cases where the genitography failed to show the vagina, we performed a cystourethroscopy and inserted a catheter inside the vagina, then we injected the contrast through it to evaluate the vaginal dimensions, the confluence depth, and the length of the proximal urethra preoperatively.
We adopted the classification that describes a high UGS if the vaginal opening is above the external sphincter. As all our patients were virilized, the urethral anatomy is more similar in appearance to a male than a female urethra. When the urethra is inserted into the perineum, it resembles a bulbar urethra that bends and goes deeply inward towards the bifurcation of the corpora cavernosa. Therefore, above this bend is the external urethral sphincter. So, if the vagina in the genitogram enters the UGS above this level, it is a high UGS, and below, it is a low UGS (Figs. 2 and 3).
Fig. 2
Genitogram showing a low persistent urogenital sinus where the vaginal opening is below the urethral bend (arrow). UB, urinary bladder; V, vagina
Fig. 3
Genitogram showing a high persistent urogenital sinus
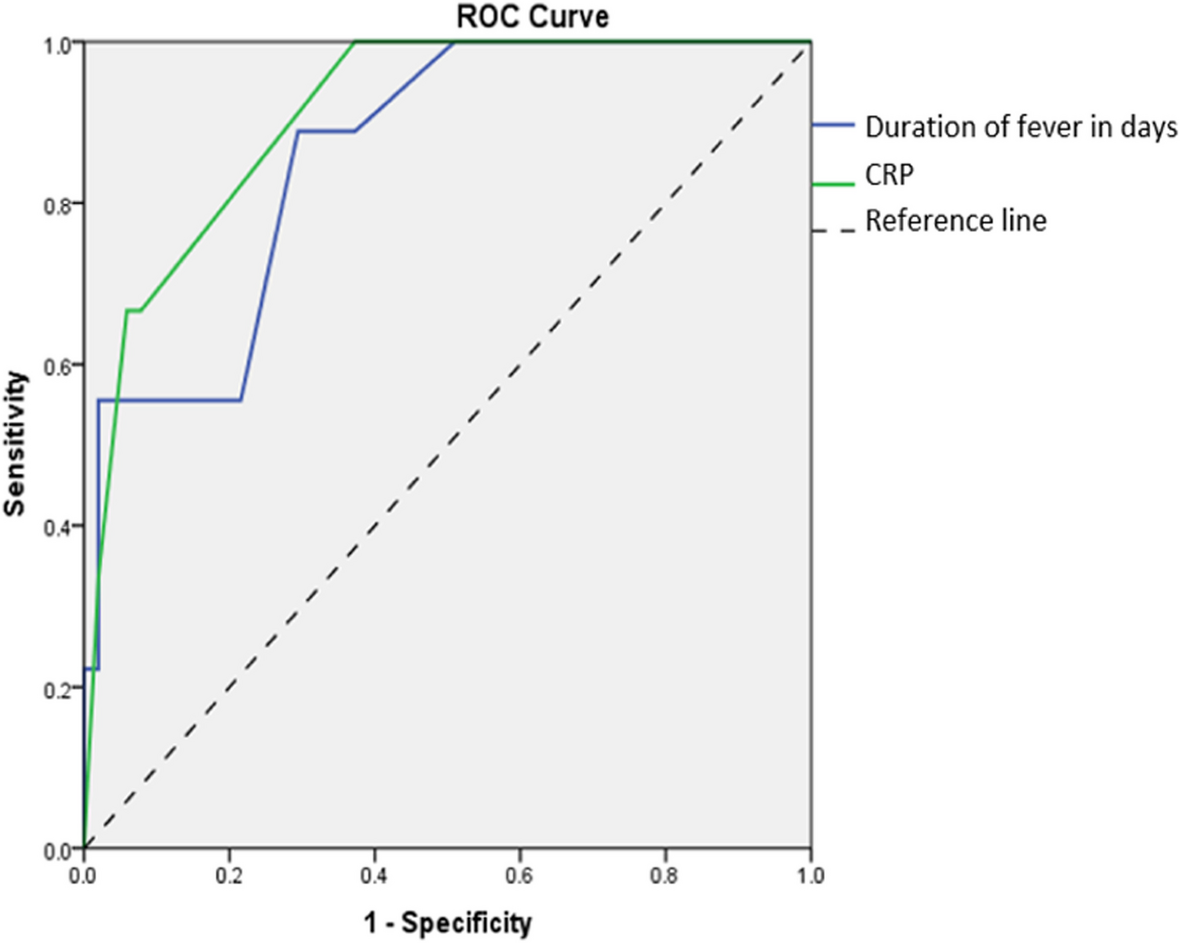
Data were coded and entered using the statistical package for the Social Sciences (SPSS) version 28 (IBM Corp., Armonk, NY, USA). Data was summarised using mean and standard deviation for normally distributed quantitative variables or median and interquartile range for non-normally distributed quantitative variables and frequencies (number of cases) and relative frequencies (percentages) for categorical variables. Comparisons between groups were done using unpaired t-test in normally distributed quantitative variables, while non-parametric Mann–Whitney test was used for non-normally distributed quantitative variables. Comparison between the length of the urethra proximal to the confluence and the expected urethral length for age in each type was done using paired t-test (Chan, 2003a). Correlations between quantitative variables were done using Spearman correlation coefficient (Chan, 2003b). ROC curve was constructed with area under curve analysis performed to detect the best cutoff value of significant parameters for detection of high type. P-values less than 0.05 were considered statistically significant.
留言 (0)